

Disparities in Excess Mortality Associated with COVID-19 - United States, 2020
- PMID: 34411075
- PMCID: PMC8375709
- DOI: 10.15585/mmwr.mm7033a2
Disparities in Excess Mortality Associated with COVID-19 - United States, 2020
Abstract
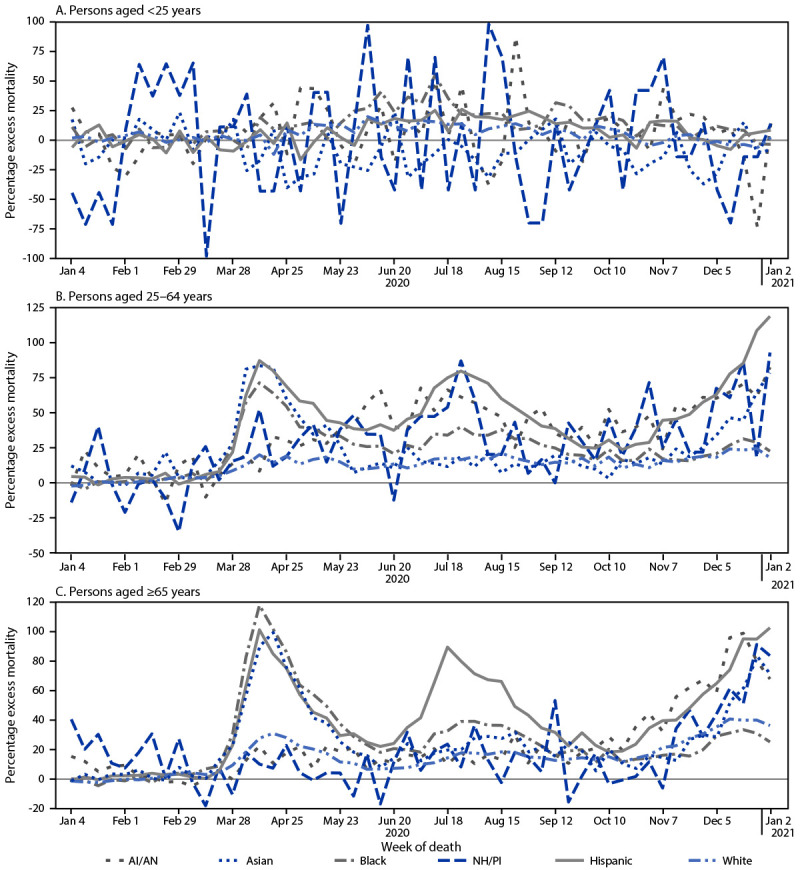
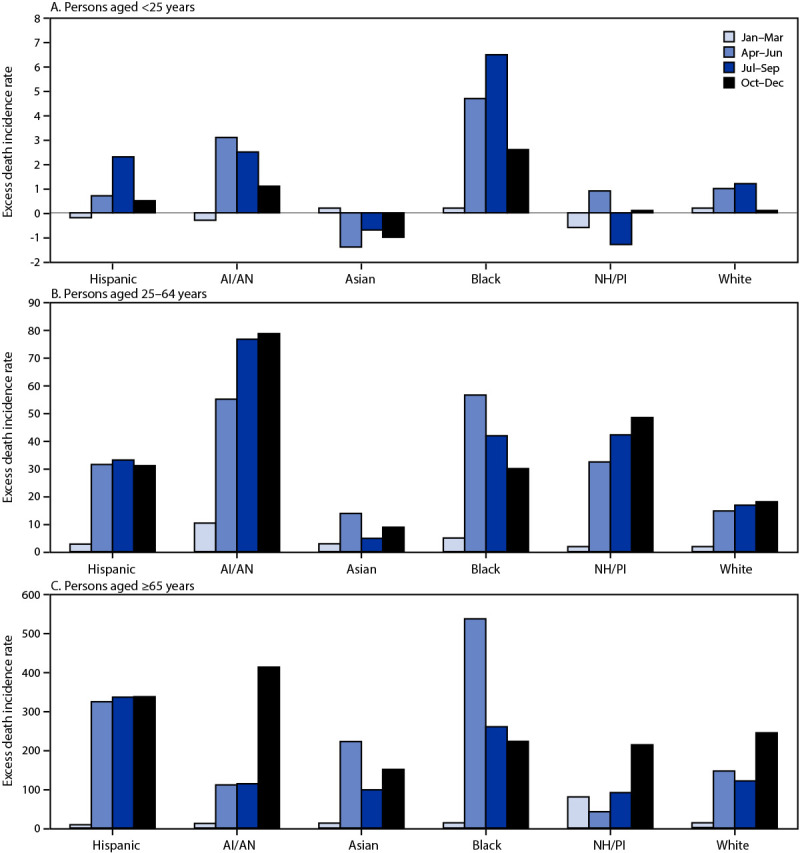
The COVID-19 pandemic has disproportionately affected Hispanic or Latino, non-Hispanic Black (Black), non-Hispanic American Indian or Alaska Native (AI/AN), and non-Hispanic Native Hawaiian or Other Pacific Islander (NH/PI) populations in the United States. These populations have experienced higher rates of infection and mortality compared with the non-Hispanic White (White) population (1-5) and greater excess mortality (i.e., the percentage increase in the number of persons who have died relative to the expected number of deaths for a given place and time) (6). A limitation of existing research on excess mortality among racial/ethnic minority groups has been the lack of adjustment for age and population change over time. This study assessed excess mortality incidence rates (IRs) (e.g., the number of excess deaths per 100,000 person-years) in the United States during December 29, 2019-January 2, 2021, by race/ethnicity and age group using data from the National Vital Statistics System. Among all assessed racial/ethnic groups (non-Hispanic Asian [Asian], AI/AN, Black, Hispanic, NH/PI, and White populations), excess mortality IRs were higher among persons aged ≥65 years (426.4 to 1033.5 excess deaths per 100,000 person-years) than among those aged 25-64 years (30.2 to 221.1) and those aged <25 years (-2.9 to 14.1). Among persons aged <65 years, Black and AI/AN populations had the highest excess mortality IRs. Among adults aged ≥65 years, Black and Hispanic persons experienced the highest excess mortality IRs of >1,000 excess deaths per 100,000 person-years. These findings could help guide more tailored public health messaging and mitigation efforts to reduce disparities in mortality associated with the COVID-19 pandemic in the United States,* by identifying the racial/ethnic groups and age groups with the highest excess mortality rates.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. Zhenqiu Lin reports contract support from the Centers for Medicare & Medicaid Services (CMS) to develop and maintain measures of hospital performance that are publicly reported. Harlan M. Krumholz reports the following outside the current work: honoraria for presentations at various educational events; grants from Medtronic and the Food and Drug Administration, Medtronic and Johnson & Johnson, Shenzhen Center for Health Information, Foundation for a Smoke-Free World, and Connecticut Department of Public Health and CMS; payment from law firms Martin/Baughman, Arnold & Porter, and Siegfried & Jensen for expert testimony; chairmanship or member of United Healthcare cardiac scientific advisory board, IBM Watson Health life sciences board, Element Science scientific advisor, Aetna health care advisory board, and Facebook advisory board; and ownership of Hugo Health and Refractor Health. No other potential conflicts of interest were disclosed.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
