

Anakinra for palmoplantar pustulosis: results from a randomized, double-blind, multicentre, two-staged, adaptive placebo-controlled trial (APRICOT)
- PMID: 34411292
- PMCID: PMC9255857
- DOI: 10.1111/bjd.20653
Anakinra for palmoplantar pustulosis: results from a randomized, double-blind, multicentre, two-staged, adaptive placebo-controlled trial (APRICOT)
Abstract
Background: Palmoplantar pustulosis (PPP) is a rare, debilitating, chronic inflammatory skin disease that affects the hands and feet. Clinical, immunological and genetic findings suggest a pathogenic role for interleukin (IL)-1.
Objectives: To determine whether anakinra (an IL-1 receptor antagonist) delivers therapeutic benefit in PPP.
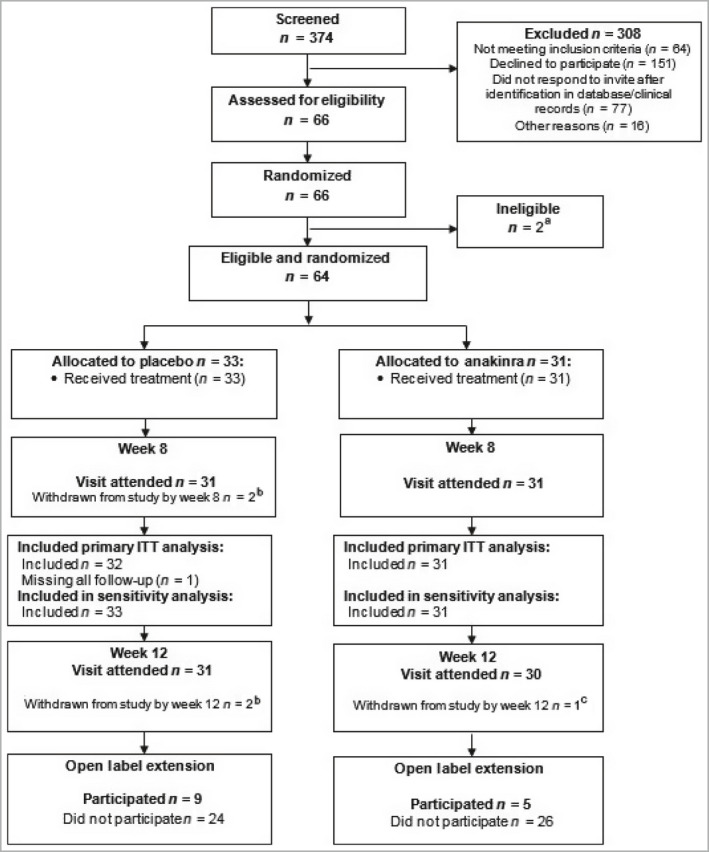
Methods: This was a randomized (1 : 1), double-blind, two-staged, adaptive, UK multicentre, placebo-controlled trial [ISCRTN13127147 (registered 1 August 2016); EudraCT number: 2015-003600-23 (registered 1 April 2016)]. Participants had a diagnosis of PPP (> 6 months) requiring systemic therapy. Treatment was 8 weeks of anakinra or placebo via daily, self-administered subcutaneous injections. Primary outcome was the Palmoplantar Pustulosis Psoriasis Area and Severity Index (PPPASI) at 8 weeks.
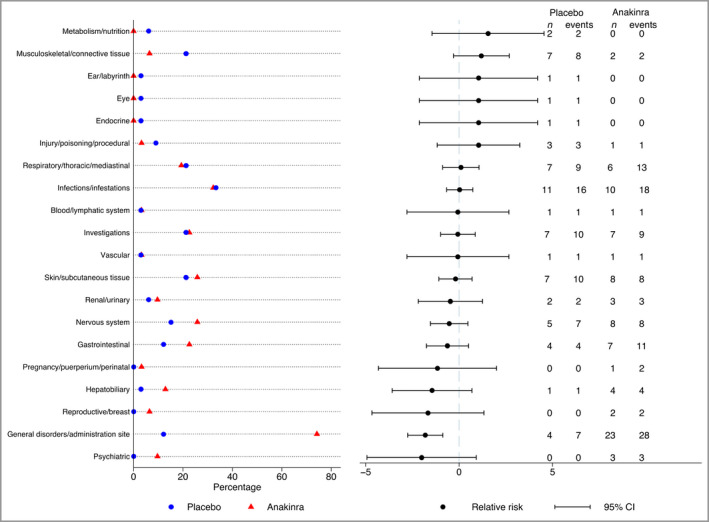
Results: A total of 374 patients were screened; 64 were enrolled (31 in the anakinra arm and 33 in the placebo arm) with a mean (SD) baseline PPPASI of 17·8 (10·5) and a PPP investigator's global assessment of severe (50%) or moderate (50%). The baseline adjusted mean difference in PPPASI favoured anakinra but did not demonstrate superiority in the intention-to-treat analysis [-1·65, 95% confidence interval (CI) -4·77 to 1·47; P = 0·30]. Similarly, secondary objective measures, including fresh pustule count (2·94, 95% CI -26·44 to 32·33; favouring anakinra), total pustule count (-30·08, 95% CI -83·20 to 23·05; favouring placebo) and patient-reported outcomes, did not show superiority of anakinra. When modelling the impact of adherence, the PPPASI complier average causal effect for an individual who received ≥ 90% of the total treatment (48% in the anakinra group) was -3·80 (95% CI -10·76 to 3·16; P = 0·285). No serious adverse events occurred.
Conclusions: No evidence for the superiority of anakinra was found. IL-1 blockade is not a useful intervention for the treatment of PPP.
© 2021 British Association of Dermatologists.
Figures

Comment in
-
Adaptive designs for clinical trials have potential advantages, but statistical challenges lurk!Br J Dermatol. 2022 Feb;186(2):205-206. doi: 10.1111/bjd.20828. Epub 2021 Nov 22. Br J Dermatol. 2022. PMID: 34806162 No abstract available.
-
Response to: 'Anakinra for palmoplantar pustulosis: results from a randomized, double-blind, multicentre, two-staged, adaptive placebo-controlled trial (APRICOT)': reply from the authors.Br J Dermatol. 2022 May;186(5):909-910. doi: 10.1111/bjd.20944. Epub 2022 Mar 2. Br J Dermatol. 2022. PMID: 34878650
-
Response to 'Anakinra for palmoplantar pustulosis: results from a randomized, double-blind, multicentre, two-staged, adaptive placebo-controlled trial (APRICOT)'.Br J Dermatol. 2022 May;186(5):908. doi: 10.1111/bjd.20942. Epub 2022 Apr 8. Br J Dermatol. 2022. PMID: 34878653 No abstract available.
References
-
- Navarini AA, Burden AD, Capon F et al. European consensus statement on phenotypes of pustular psoriasis. J Eur Acad Dermatol Venereol 2017; 31:1792–9. - PubMed
-
- National Health Service Psoriasis – overview. Available at: https://www.nhs.uk/conditions/psoriasis/ (last accessed 29 October 2020).
-
- Griffiths CE, Christophers E, Barker JN et al. A classification of psoriasis vulgaris according to phenotype. Br J Dermatol 2007; 156:258–62. - PubMed
-
- Bhutani T, Patel T, Koo B et al. A prospective, interventional assessment of psoriasis quality of life using a nonskin‐specific validated instrument that allows comparison with other major medical conditions. J Am Acad Dermatol 2013; 69:e79–88. - PubMed
-
- Sampogna F, Gisondi P, Melchi CF et al. Prevalence of symptoms experienced by patients with different clinical types of psoriasis. Br J Dermatol 2004; 151:594–9. - PubMed
Grants and funding
- NIHR EME 13/50/17 APRICOT/Efficacy and Mechanism Evaluation Programme
- RG2/10/The Psoriasis Association
- guysbrc-2012-1/NIHR BioResource Clinical Research Facility and comprehensive Biomedical Research Centre awards to Guy's and St Thomas' NHS Foundation Trust in partnership with King's College London and King's College Hospital NHS Foundation Trust
- Swedish Orphan Biovitrum
