

Cesarean delivery rates, hospital readiness and quality of clinical management in Ethiopia: national results from two cross-sectional emergency obstetric and newborn care assessments
- PMID: 34412599
- PMCID: PMC8377989
- DOI: 10.1186/s12884-021-04008-9
Cesarean delivery rates, hospital readiness and quality of clinical management in Ethiopia: national results from two cross-sectional emergency obstetric and newborn care assessments
Abstract
Background: Cesarean delivery (CD) rates have reached epidemic levels in many high and middle income countries while increasingly, low income countries are challenged both by high urban CD rates and high unmet need in rural areas. The managing authority of health care institutions often plays a role in these disparities. This paper shows changes between 2008 and 2016 in Ethiopian CD rates, readiness of hospitals to provide CD and quality of clinical care, while highlighting the role of hospital management authority.
Methods: This secondary data analysis draws from two national cross-sectional studies to assess emergency obstetric and newborn care. The sample includes 111 hospitals in 2008 and 316 hospitals in 2016, and 275 women whose CD chart was reviewed in 2008 and 568 in 2016. Descriptive statistics are used to describe our primary outcome measures: population- and institutional-based CD rates; hospital readiness to perform CD; quality of clinical management, including the relative size of Robson classification groups.
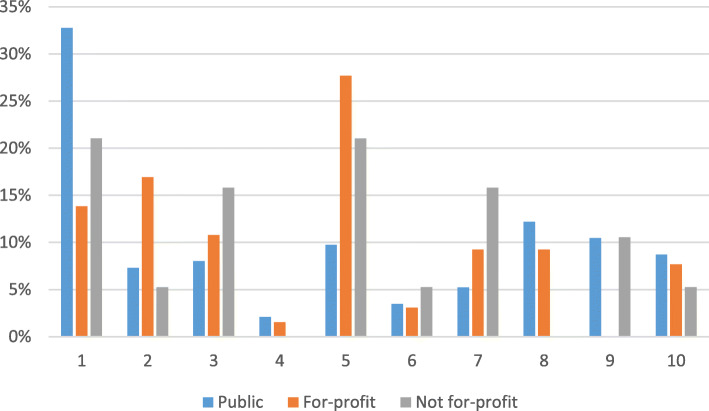
Results: The national population CD rate increased from 2008 to 2016 (< 1 to 2.7%) as did all regional rates. Rates in 2016 ranged from 24% in urban settings to less than 1% in several rural regions. The institutional rate was 54% in private for-profit hospitals in 2016, up from 46% in 2008. Hospital readiness to perform CDs increased in public and private for-profit hospitals. Only half of the women whose charts were reviewed received uterotonics after delivery of the baby, but use of prophylactic antibiotics was high. Partograph use increased from 9 to 42% in public hospitals, but was negligible or declined elsewhere. In 2016, 40% of chart reviews from public hospitals were among low-risk nulliparous women (Robson groups 1&2).
Conclusions: Between 2008 and 2016, government increased the availability of CD services, improved public hospital readiness and some aspects of clinical quality. Strategies tailored to further reduce the high unmet need for CD and what appears to be an increasing number of unnecessary cesareans are discussed. Adherence to best practices and universal coverage of water and electricity will improve the quality of hospital services while the use of the Robson classification system may serve as a useful quality improvement tool.
Keywords: Cesarean delivery; Cesarean rates; Cesarean-section; Public/private managing authority; Quality of care; Readiness; Robson classification.
© 2021. The Author(s).
Conflict of interest statement
None of the authors has any competing interests.
Figures
References
-
- Miller S, Abalos E, Chamillard M, Ciapponi A, Colaci D, Comande D, Diaz V, Geller S, Hanson C, Langer A, et al. Beyond too little, too late and too much, too soon: a pathway towards evidence-based, respectful maternity care worldwide. Lancet. 2016;388(10056):2176–2192. doi: 10.1016/S0140-6736(16)31472-6. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
