

Feasibility and implementation of a personalized, web-based exercise intervention for people with cystic fibrosis for 1 year
- PMID: 34412703
- PMCID: PMC8377819
- DOI: 10.1186/s13102-021-00323-y
Feasibility and implementation of a personalized, web-based exercise intervention for people with cystic fibrosis for 1 year
Abstract
Background: Regular participation in exercise is important for people with cystic fibrosis (CF). Therefore, we implemented a personalized, web-based exercise intervention over the course of one year for people with CF. The aims were to investigate the feasibility of the intervention and to evaluate changes in exercise participation, lung function, and exercise capacity.
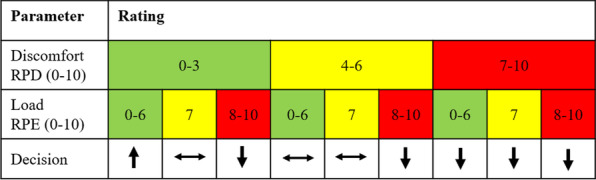
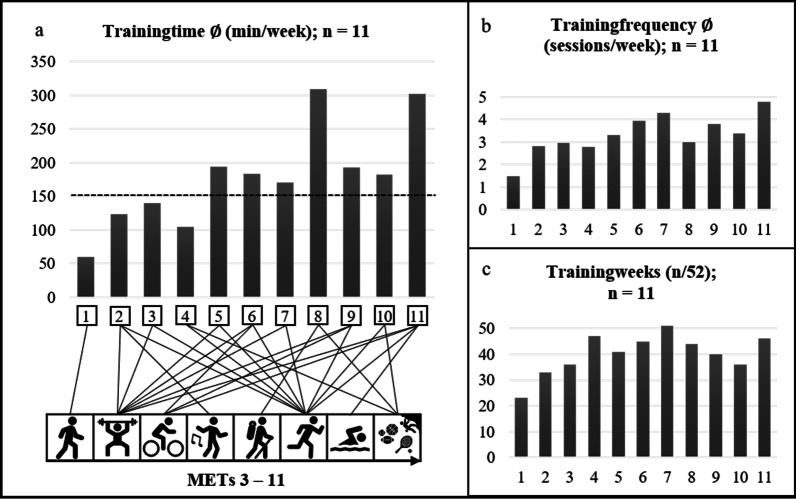
Methods: In total, 11/17 participants [aged 12-52 years; FEV1%pred. 72.3 (SD: 17.3)] were included in the final data analysis. Every week, the participants received an individual training recommendation at the start and uploaded their training report on our website at the end of each week. The number of training minutes and sessions performed were analyzed over 13 four-week training sections. The participation in exercise (physical activity questionnaire), lung function and exercise capacity were assessed at baseline (T0), after 12 weeks (T1) and after 52 weeks (T2).
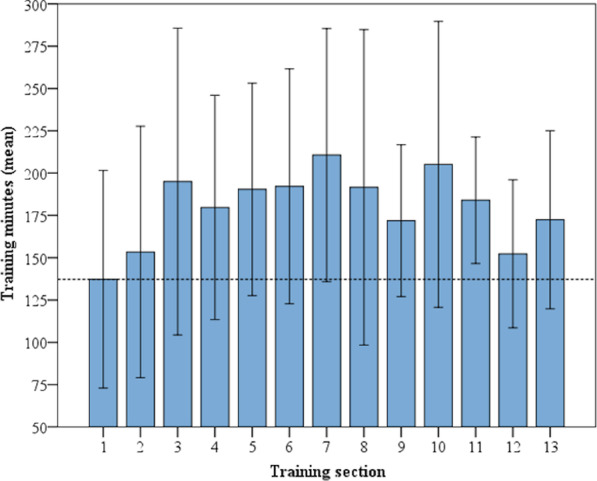
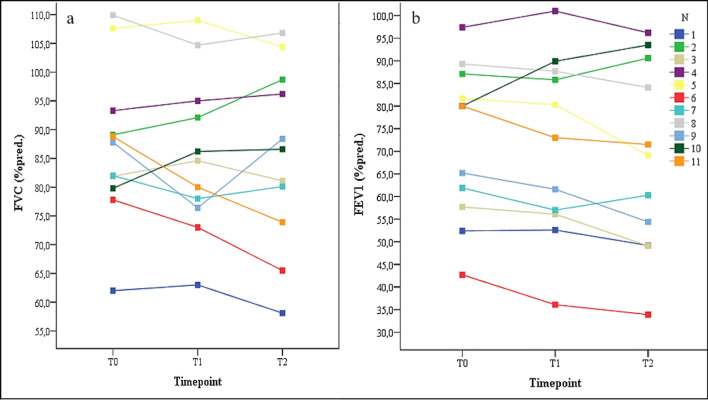
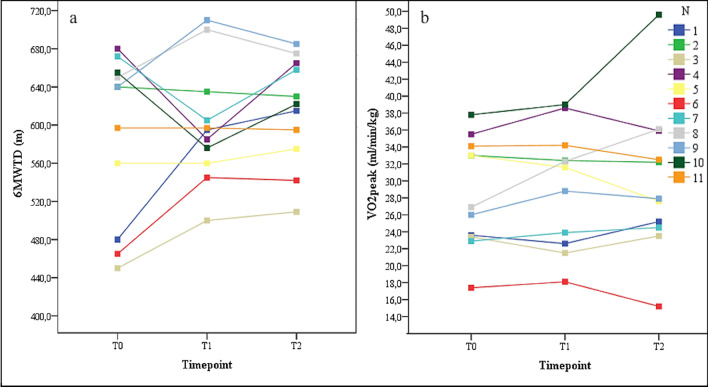
Results: A training duration of 178 min (SD: 75.5) and 3.3 (SD: 0.89) training sessions could be achieved weekly. In the first four-week training section, the participants performed 137.31 (SD: 95.7) minutes of training, with an increase of 42% in the third training section (195.01, SD: 134.99). Minutes of training reported on the questionnaire increased by 39.7% from T0 (179.38 min, SD: 120.9) to T1 (250.63 min, SD: 124.1) but decreased at T2 (166.88, SD: 155.4). There were slight decreases in lung function (FEV1 - 3.9%pred.; FVC - 1.9%pred.) and slight increases in exercise capacity (VO2peak + 1.5 ml/min/kg; six-minute-walk-test-distance + 26 m). Noticeably, five participants experienced deteriorations in their FEV1 of more than 5% but simultaneously experienced improvements in the parameters of exercise capacity of more than 5% throughout the year.
Conclusions: The web-based concept was feasible for the participants over the course of a year and supported exercise participation. The improvement in exercise capacity due to increased exercise participation over a prolonged period of time, despite a decrease in lung function, should be further investigated. Finally, if integrated into usual care, this approach could facilitate the prescription of regular personalized exercise and promote exercise participation in the daily lives of people with CF.
Keywords: Chronic diseases; Clinical exercise therapy; Exercise prescription; Long-term intervention; Personalized telemedicine.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Alack K, Pilat C, Krüger K. Current knowledge and new challenges in exercise immunology. Dtsch Z Sportmed. 2019;70(10):250–260. doi: 10.5960/dzsm.2019.391. - DOI
-
- Pedersen BK. Physical exercise in chronic diseases. Nutr Skeletal Muscle. 2019;217–66.
LinkOut - more resources
Full Text Sources
