

Oral microflora and pregnancy: a systematic review and meta-analysis
- PMID: 34413437
- PMCID: PMC8377136
- DOI: 10.1038/s41598-021-96495-1
Oral microflora and pregnancy: a systematic review and meta-analysis
Abstract
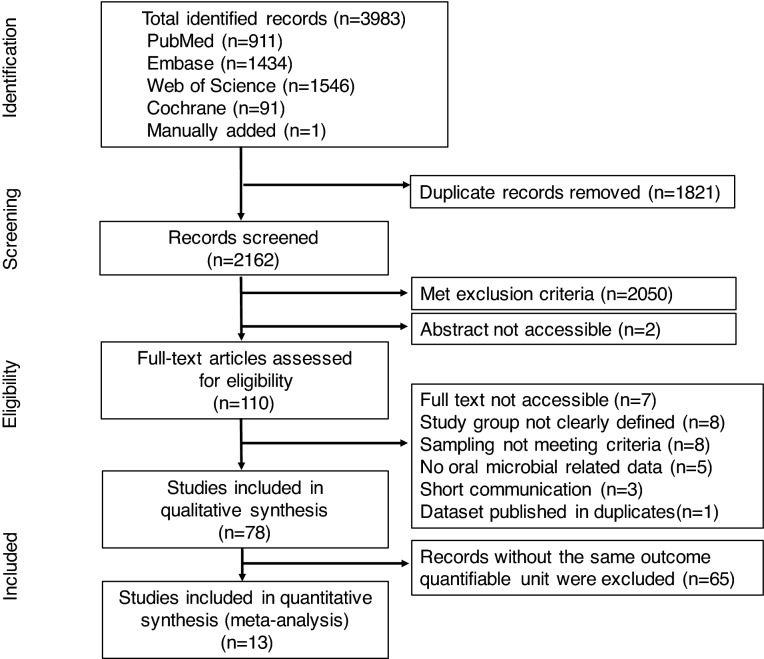
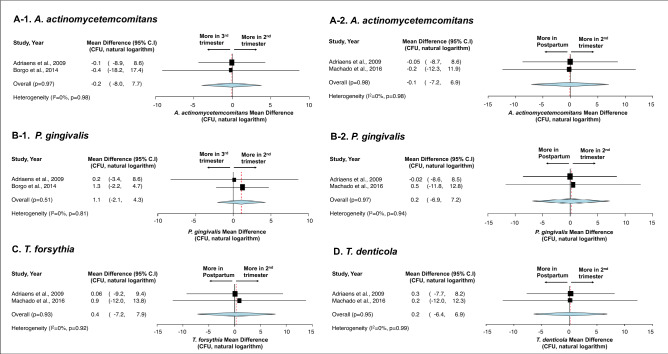
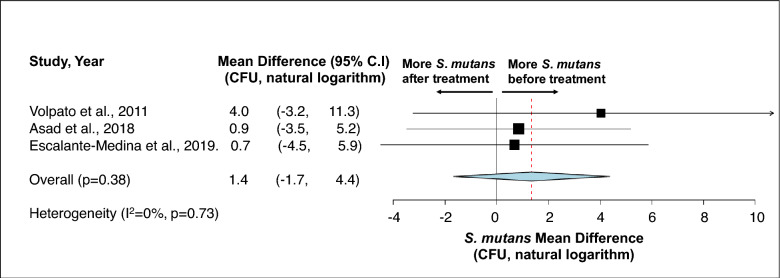
Understanding changes in oral flora during pregnancy, its association to maternal health, and its implications to birth outcomes is essential. We searched PubMed, Embase, Web of Science, and Cochrane Library in May 2020 (updated search in April and June 2021), and conducted a systematic review and meta-analyses to assess the followings: (1) oral microflora changes throughout pregnancy, (2) association between oral microorganisms during pregnancy and maternal oral/systemic conditions, and (3) implications of oral microorganisms during pregnancy on birth outcomes. From 3983 records, 78 studies were included for qualitative assessment, and 13 studies were included in meta-analysis. The oral microflora remains relatively stable during pregnancy; however, pregnancy was associated with distinct composition/abundance of oral microorganisms when compared to postpartum/non-pregnant status. Oral microflora during pregnancy appears to be influenced by oral and systemic conditions (e.g. gestational diabetes mellitus, pre-eclampsia, etc.). Prenatal dental care reduced the carriage of oral pathogens (e.g. Streptococcus mutans). The Porphyromonas gingivalis in subgingival plaque was more abundant in women with preterm birth. Given the results from meta-analyses were inconclusive since limited studies reported outcomes on the same measuring scale, more future studies are needed to elucidate the association between pregnancy oral microbiota and maternal oral/systemic health and birth outcomes.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Kandan PM, Menaga V, Kumar RRR. Oral health in pregnancy (guidelines to gynaecologists, general physicians & oral health care providers) JPMA J. Pakistan Med. Assoc. 2011;61:1009. - PubMed
-
- Neuman, H. & Koren, O. in Intestinal Microbiome: Functional Aspects in Health and Disease Vol. 88 Nestle Nutrition Institute Workshop Series (eds E. Isolauri, P. M. Sherman, & W. A. Walker) 1–9 (2017).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
