

LDL receptor-peptide conjugate as in vivo tool for specific targeting of pancreatic ductal adenocarcinoma
- PMID: 34413441
- PMCID: PMC8377056
- DOI: 10.1038/s42003-021-02508-0
LDL receptor-peptide conjugate as in vivo tool for specific targeting of pancreatic ductal adenocarcinoma
Abstract
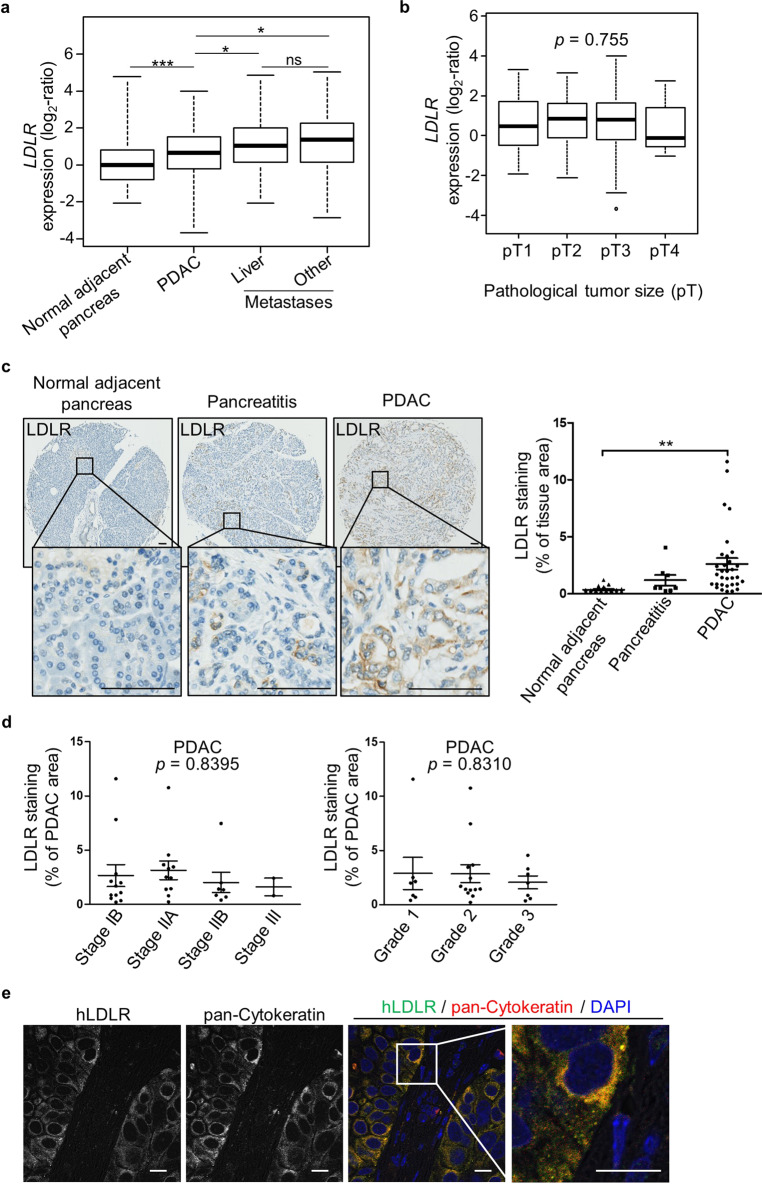
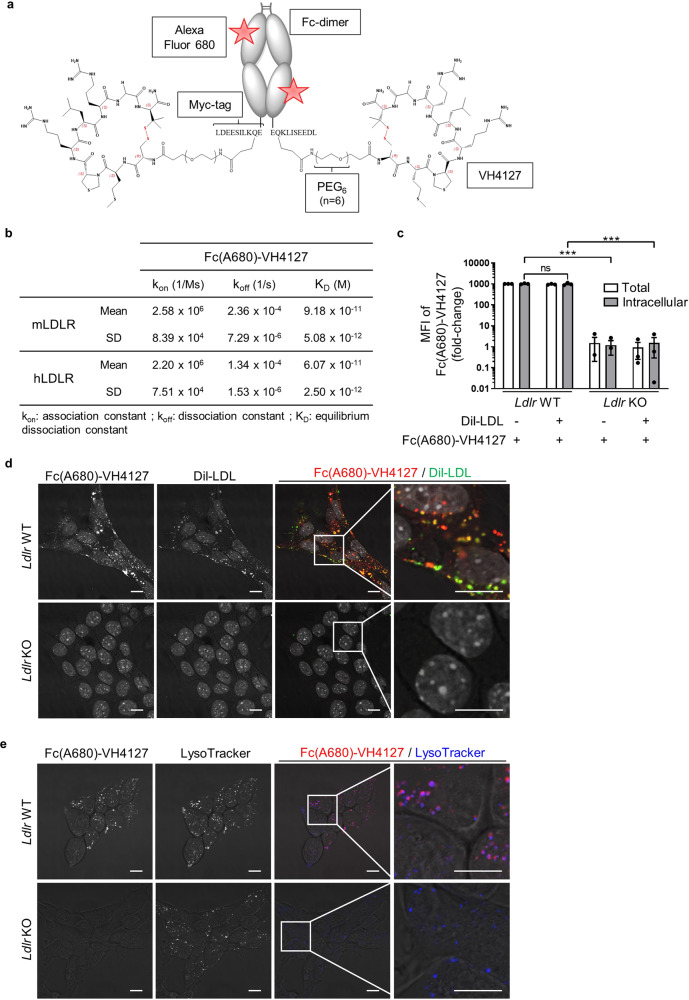
Despite clinical advances in diagnosis and treatment, pancreatic ductal adenocarcinoma (PDAC) remains the third leading cause of cancer death, and is still associated with poor prognosis and dismal survival rates. Identifying novel PDAC-targeted tools to tackle these unmet clinical needs is thus an urgent requirement. Here we use a peptide conjugate that specifically targets PDAC through low-density lipoprotein receptor (LDLR). We demonstrate by using near-infrared fluorescence imaging the potential of this conjugate to specifically detect and discriminate primary PDAC from healthy organs including pancreas and from benign mass-forming chronic pancreatitis, as well as detect metastatic pancreatic cancer cells in healthy liver. This work paves the way towards clinical applications in which safe LDLR-targeting peptide conjugate promotes tumor-specific delivery of imaging and/or therapeutic agents, thereby leading to substantial improvements of the PDAC patient's outcome.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
