

Downstaging and Resection of Initially Unresectable Hepatocellular Carcinoma with Tyrosine Kinase Inhibitor and Anti-PD-1 Antibody Combinations
- PMID: 34414120
- PMCID: PMC8339461
- DOI: 10.1159/000514313
Downstaging and Resection of Initially Unresectable Hepatocellular Carcinoma with Tyrosine Kinase Inhibitor and Anti-PD-1 Antibody Combinations
Abstract
Background: Combined therapy with tyrosine kinase inhibitors (TKIs) and anti-PD-1 antibodies has shown high tumor response rates for patients with unresectable hepatocellular carcinoma (HCC). However, using this treatment strategy to convert initially unresectable HCC to resectable HCC was not reported.
Methods: Consecutive patients with unresectable HCC who received first-line therapy with combined TKI/anti-PD-1 antibodies were analyzed. Tumor response and resectability were evaluated via imaging every 2 months (±2 weeks) using RECIST v1.1. Resectability criteria were (1) R0 resection could be achieved with sufficient remnant liver volume and function; (2) intrahepatic lesions were evaluated as partial responses or stable disease for at least 2 months; (3) no severe or persistent adverse effects occurred; and (4) hepatectomy was not contraindicated.
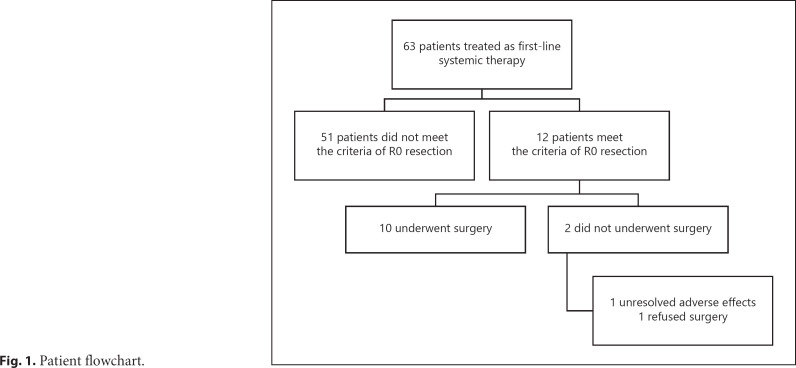
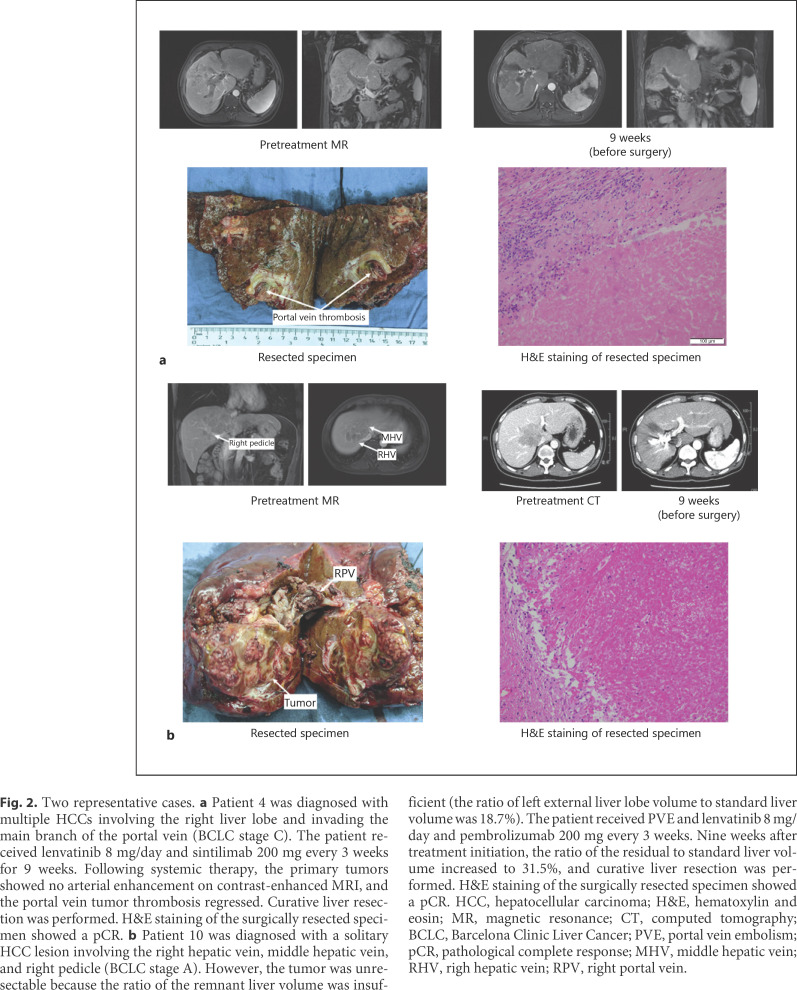
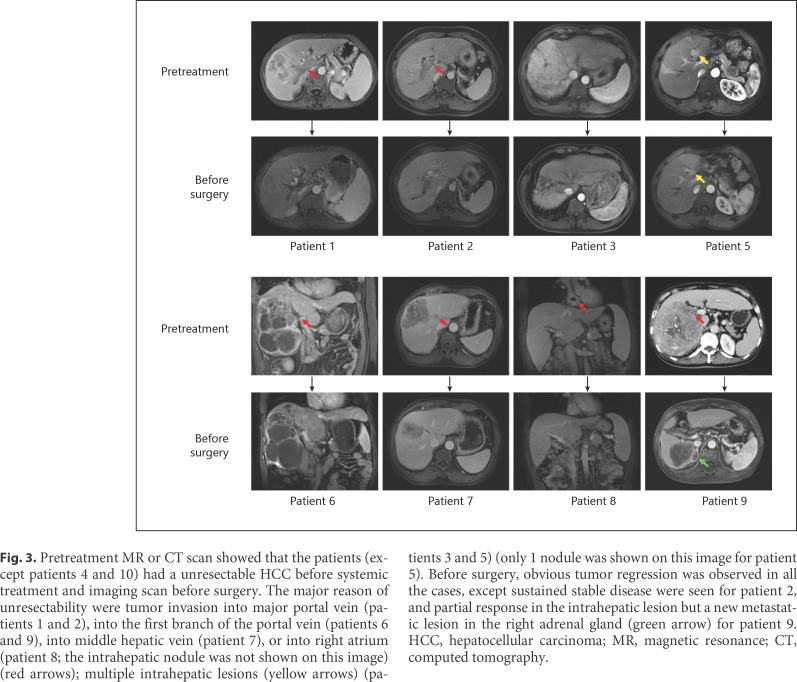
Results: Sixty-three consecutive patients were enrolled. Of them, 10 (15.9%) underwent R0 resection in 3.2 months (range: 2.4-8.3 months) after the initiation of combination therapy. At baseline, these 10 patients had a median largest tumor diameter of 9.3 cm, 7 had Barcelona Clinic Liver Cancer stage C (vascular invasion) disease, 2 had stage B, and 1 had stage A. Before surgery, 6 patients were evaluated as a partial response, 3 stable disease, and 1 partial response in the intrahepatic lesion but a new metastatic lesion in the right adrenal gland. Six patients (60%) achieved a pathological complete response. One patient died from immune-related adverse effects 2.4 months after hepatectomy. After a median follow-up of 11.2 months (range: 7.8-15.9 months) for other 9 patients, 8 survived without disease recurrence, and 1 experienced tumor recurrence.
Conclusions: Combination of TKI/anti-PD-1 antibodies is a feasible conversion therapy for patients with unresectable HCC to become resectable. This study represents the largest patient cohort on downstaging role of combinational systemic therapy on TKI and PD-1 antibody for HCC.
Keywords: Anti-PD-1 antibody; Anti-angiogenic therapy; Conversion therapy; Hepatocellular carcinoma.
Copyright © 2021 by S. Karger AG, Basel.
Conflict of interest statement
H.C.S. has received speaker fees from Hengrui, Bayer, Eisai, and MSD. X.D.Z. has received speaker fees from Eisai and MSD. Dr. Jia Fan is an Editorial Board Member of Liver Cancer.
Figures
References
-
- Zhou M, Wang H, Zhu J, Chen W, Wang L, Liu S, et al. Cause-specific mortality for 240 causes in China during 1990–2013: a systematic subnational analysis for the Global Burden of Disease Study 2013. Lancet. 2016;387((10015)):251–72. - PubMed
-
- Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66((2)):115–32. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2019;66((1)):7–30. - PubMed
LinkOut - more resources
Full Text Sources
Medical
