

European Stroke Organisation guideline on endarterectomy and stenting for carotid artery stenosis
- PMID: 34414302
- PMCID: PMC8370069
- DOI: 10.1177/23969873211012121
European Stroke Organisation guideline on endarterectomy and stenting for carotid artery stenosis
Abstract
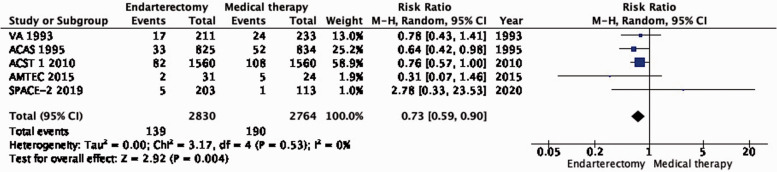
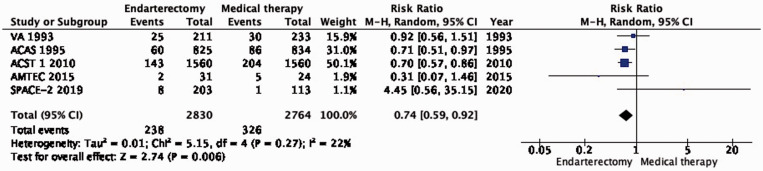
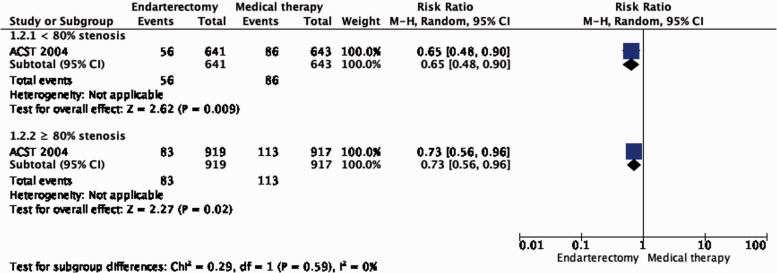
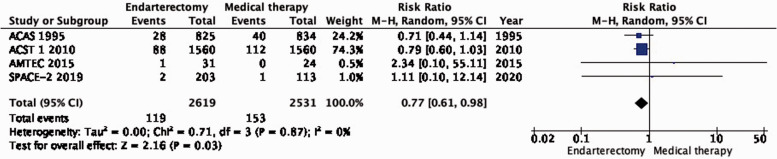
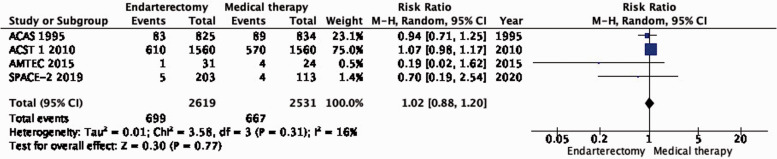
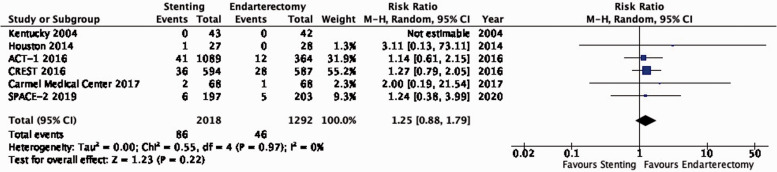
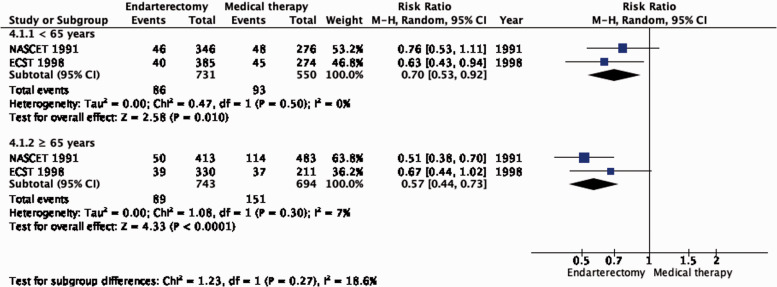
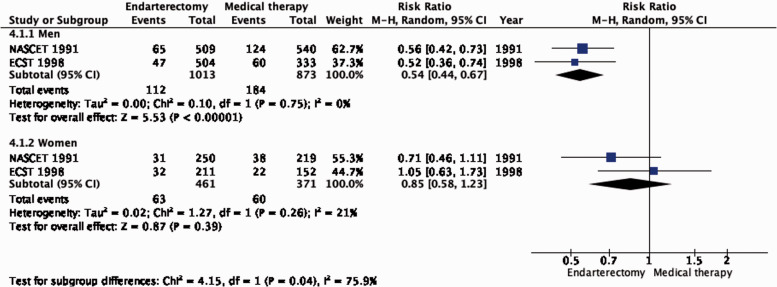
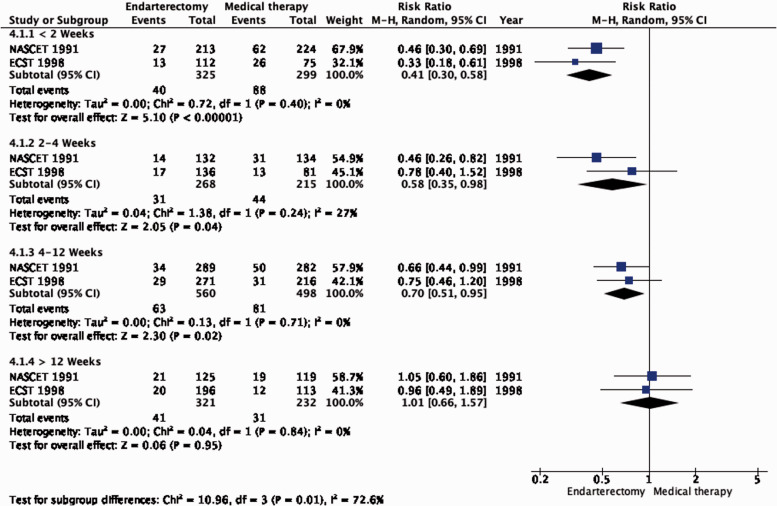
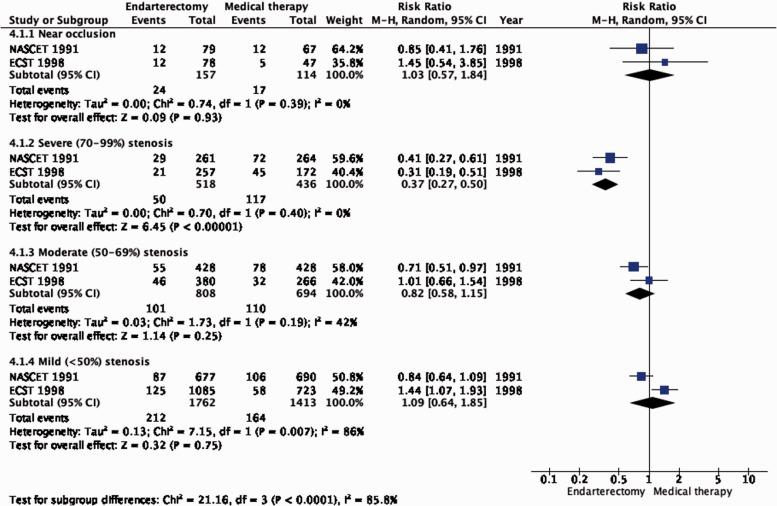
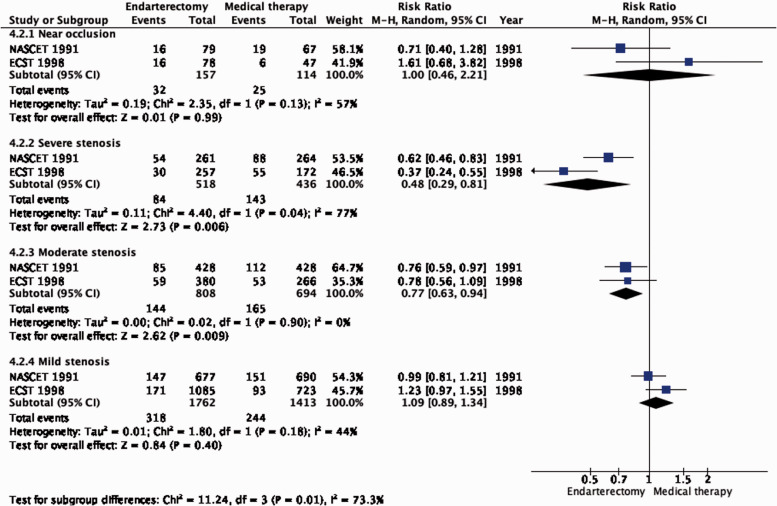
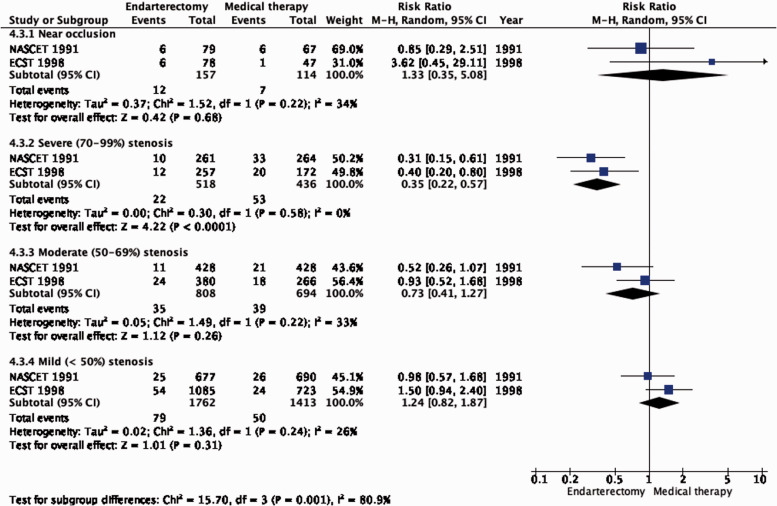
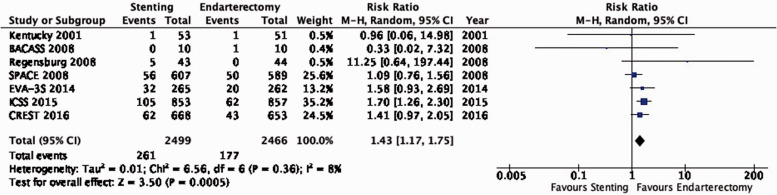
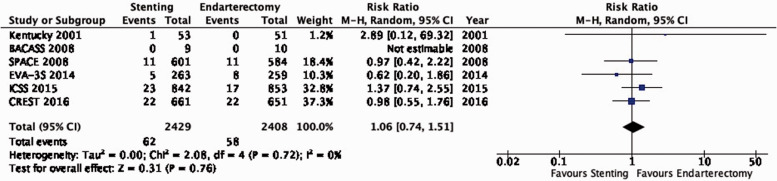
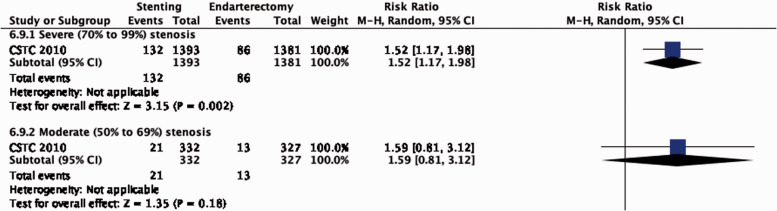
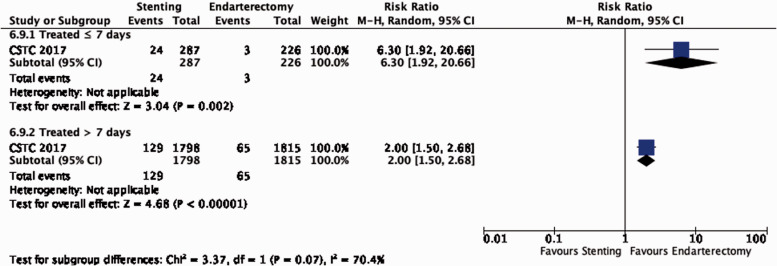
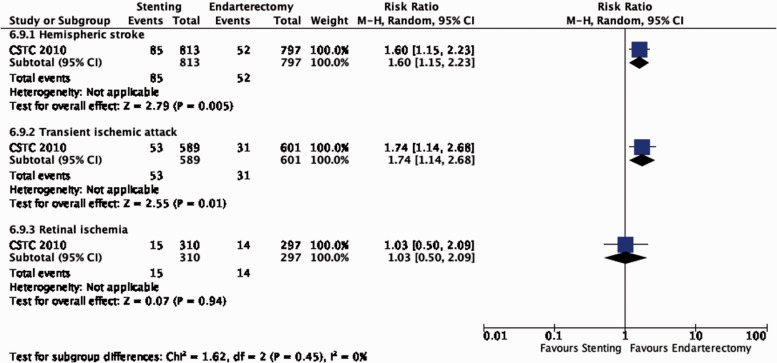
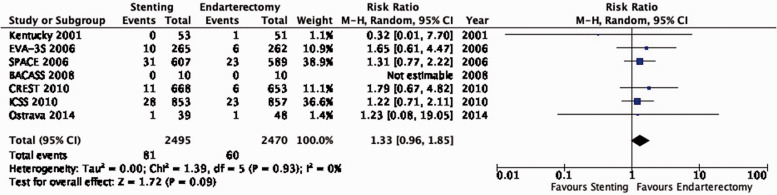
Atherosclerotic stenosis of the internal carotid artery is an important cause of stroke. The aim of this guideline is to analyse the evidence pertaining to medical, surgical and endovascular treatment of patients with carotid stenosis. These guidelines were developed based on the ESO standard operating procedure and followed the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach. The working group identified relevant questions, performed systematic reviews and meta-analyses of the literature, assessed the quality of the available evidence, and wrote recommendations. Based on moderate quality evidence, we recommend carotid endarterectomy (CEA) in patients with ≥60-99% asymptomatic carotid stenosis considered to be at increased risk of stroke on best medical treatment (BMT) alone. We also recommend CEA for patients with ≥70-99% symptomatic stenosis, and we suggest CEA for patients with 50-69% symptomatic stenosis. Based on high quality evidence, we recommend CEA should be performed early, ideally within two weeks of the last retinal or cerebral ischaemic event in patients with ≥50-99% symptomatic stenosis. Based on low quality evidence, carotid artery stenting (CAS) may be considered in patients < 70 years old with symptomatic ≥50-99% carotid stenosis. Several randomised trials supporting these recommendations were started decades ago, and BMT, CEA and CAS have evolved since. The results of another large trial comparing outcomes after CAS versus CEA in patients with asymptomatic stenosis are anticipated in the near future. Further trials are needed to reassess the benefits of carotid revascularisation in combination with modern BMT in subgroups of patients with carotid stenosis.
Keywords: Carotid stenosis; endarterectomy; medical therapy; stenting; stroke; transient ischaemic attack.
© European Stroke Organisation 2021.
Figures











Comment in
-
ESO-Leitlinie Carotisstenose.Rofo. 2022 Mar;194(3):327-328. doi: 10.1055/a-1720-6476. Epub 2022 Feb 11. Rofo. 2022. PMID: 35148555 German. No abstract available.
References
-
- Petty GW, Brown RD, Jr, Whisnant JP, et al.. Ischemic stroke subtypes: a population-based study of incidence and risk factors. Stroke 1999; 30: 2513–2516. - PubMed
-
- Fisher CM, Gore I, Okabe N, et al.. Atherosclerosis of the carotid and vertebral arteries—extracranial and intracranial. J Neuropathol Exp Neurol 1965; 24: 455–476.
-
- Naylor AR, Ricco JB, de Borst GJ, et al.. Editor’s choice – management of atherosclerotic carotid and vertebral artery disease: 2017 clinical practice guidelines of the European society for vascular surgery (ESVS). Eur J Vasc Endovasc Surg 2018; 55: 3–81. - PubMed
-
- Aboyans V, Ricco JB, Bartelink MEL, et al..; ESC Scientific Document Group. 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European society for vascular surgery (ESVS): document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries. Endorsed by: the European stroke organization (ESO) the task force for the diagnosis and treatment of peripheral arterial diseases of the European society of cardiology (ESC) and of the European society for vascular surgery (ESVS). Eur Heart J 2018; 39: 763–816. - PubMed
LinkOut - more resources
Full Text Sources
Medical
