

Hospitalization-Associated Disability After Cardiac Surgery in Elderly Patients - Exploring the Risk Factors Using Machine Learning Algorithms
- PMID: 34414331
- PMCID: PMC8338437
- DOI: 10.1253/circrep.CR-21-0057
Hospitalization-Associated Disability After Cardiac Surgery in Elderly Patients - Exploring the Risk Factors Using Machine Learning Algorithms
Abstract
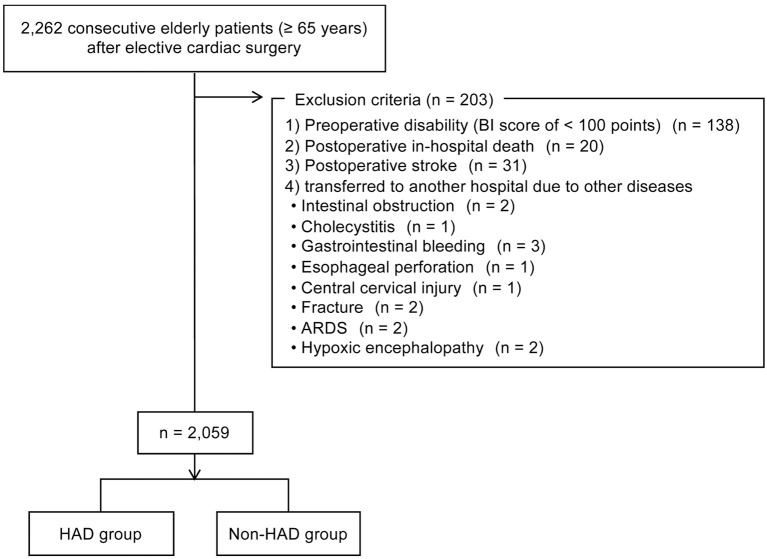
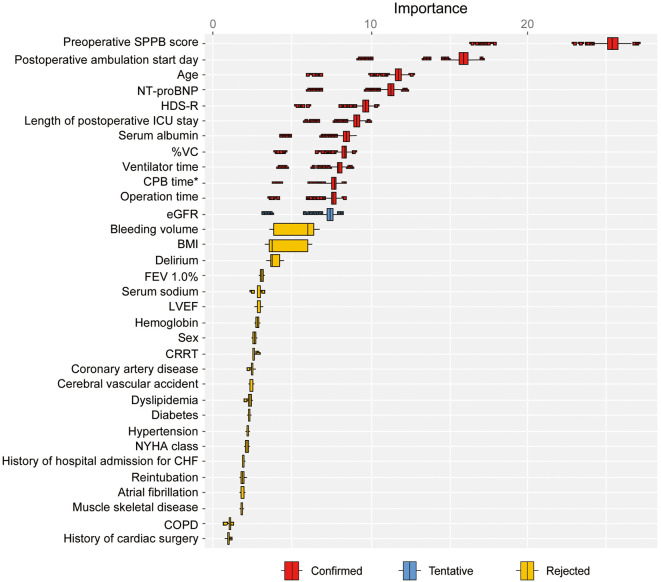
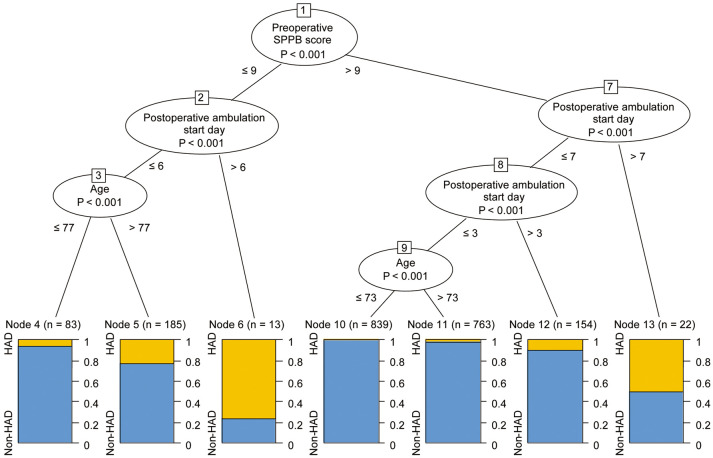
Background: Hospitalization-associated disability (HAD) is associated with prolonged functional decline and increased mortality after discharge. Therefore, we examined the incidence and risk factors associated with HAD in elderly patients undergoing cardiac surgery in Japan. Methods and Results: We retrospectively examined 2,262 elderly patients who underwent elective cardiac surgery at Sakakibara Heart Institute. HAD was defined as a functional decline between time of admission and discharge measured by the Barthel Index. We analyzed clinical characteristics using machine learning algorithms to identify the risk factors associated with HAD. After excluding 203 patients, 2,059 patients remained, of whom 108 (5.2%) developed HAD after cardiac surgery. The risk factors identified were age, serum albumin concentration, estimated glomerular filtration rate, Revised Hasegawa's Dementia Scale, N-terminal pro B-type natriuretic peptide, vital capacity, preoperative Short Physical Performance Battery (SPPB) score, operation times, cardiopulmonary bypass times, ventilator times, length of postoperative intensive care unit stay, and postoperative ambulation start day. The highest incidence of HAD was found in patients with an SPPB score ≤9 and in those who started ambulation >6 days after surgery (76.9%). Conclusions: Several risk factors for HAD are components of frailty, suggesting that preoperative rehabilitation to reduce the risk of HAD is feasible. Furthermore, the association between HAD and a delayed start of ambulation reaffirms the importance of early mobilization and rehabilitation.
Keywords: Cardiac surgery; Elderly patients; Hospitalization-associated disability; Machine learning algorithms; Risk factor.
Copyright © 2021, THE JAPANESE CIRCULATION SOCIETY.
Conflict of interest statement
T.S. is a member of Circulation Reports’ Editorial Team. K.U. is currently employed at Syneos Health and all relevant work in this manuscript was completed during his previous employment at the Hospital for Sick Children and Laurentian University. The remaining authors have no conflicts of interest to declare.
Figures
References
-
- JCS/JACR 2021 guideline on rehabilitation in patients with cardiovascular disease [in Japanese]. https://www.j-circ.or.jp/cms/wp-content/uploads/2021/03/JCS2021_Makita.pdf (accessed June 28, 2021).
-
- Covinsky KE, Pierluissi E, Johnston CB.. Hospitalization-associated disability: “She was probably able to ambulate, but I’m not sure”. JAMA 2011; 306: 1782–1793. - PubMed
-
- Fortinsky RH, Covinsky KE, Palmer RM, Landefeld CS.. Effects of functional status changes before and during hospitalization on nursing home admission of older adults. J Gerontol A Biol Sci Med Sci 1999; 54: M521–M526. - PubMed