

Thrombotic microangiopathy following aortic surgery with hypothermic circulatory arrest: a single-centre experience of an underestimated cause of acute renal failure
- PMID: 34414411
- PMCID: PMC8929442
- DOI: 10.1093/icvts/ivab231
Thrombotic microangiopathy following aortic surgery with hypothermic circulatory arrest: a single-centre experience of an underestimated cause of acute renal failure
Abstract
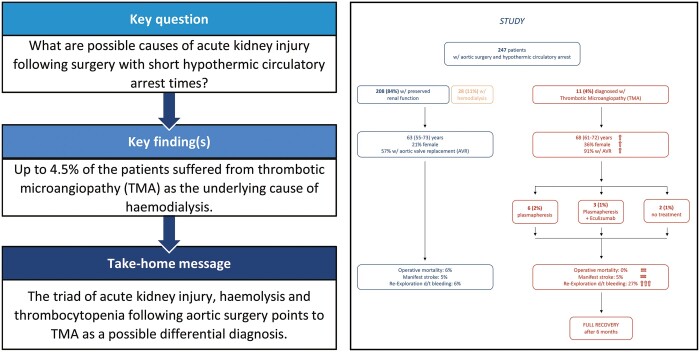
Objectives: Acute kidney injury (AKI) following surgery involving the heart-lung-machine is associated with high mortality and morbidity. In addition to the known mechanisms, thrombotic microangiopathy (TMA) triggered by the dysregulation of complement activation was recently described as another pathophysiological pathway for AKI following aortic surgery. The aim of this retrospective study was to analyse incidence, predictors and outcome in these patients.
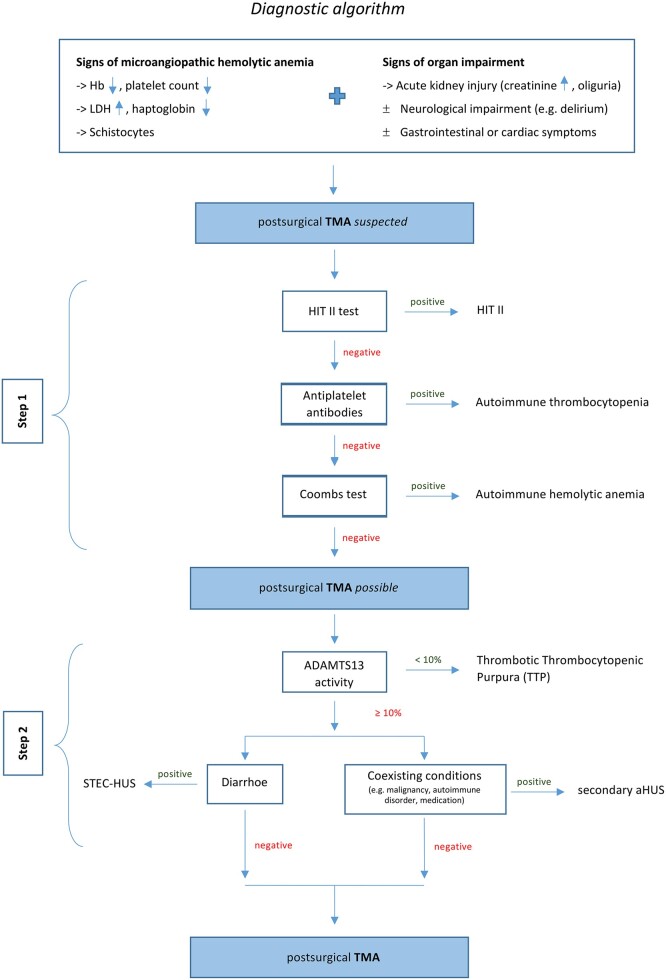
Methods: Between January 2018 and September 2019, consecutive patients undergoing aortic surgery requiring hypothermic circulatory arrest were retrospectively reviewed. If suspected, diagnostic algorithm was initiated to identify a TMA and its risk factors, and postoperative outcome parameters were comparably investigated.
Results: The incidence of TMA in the analysed cohort (n = 247) was 4.5%. Multivariable logistic regression indicated female gender {odds ratio (OR) 4.905 [95% confidence interval (CI) 1.234-19.495], P = 0.024} and aortic valve replacement [OR 8.886 (95% CI 1.030-76.660), P = 0.047] as independent predictors of TMA, while cardiopulmonary bypass, X-clamp and hypothermic circulatory arrest times showed no statistically significance. TMA resulted in postoperative AKI (82%), neurological disorders (73%) and thrombocytopaenia [31 (interquartile range 25-42) G/l], corresponding to the diagnostic criteria. Operative mortality and morbidity were equal to patients without postoperative TMA, despite a higher incidence of re-exploration for bleeding (27 vs 6%; P = 0.027). After 6 months, survival, laboratory parameters and need for dialysis were comparable between the groups.
Conclusions: TMA is a potential differential diagnosis for the cause of AKI following aortic surgery regardless of the hypothermic circulatory arrest time. Timely diagnosis and appropriate treatment resulted in a comparable outcome concerning mortality and renal function.
Keywords: Acute kidney injury; Aortic surgery; Cardiopulmonary bypass; Eculizumab; Haemolytic anaemia; Haemolytic uraemic syndrome; Hypothermic circulatory arrest; Thrombocytopaenia; Thrombotic microangiopathy.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery. All rights reserved.
Figures
References
-
- Arnaoutakis GJ, Bihorac A, Martin TD, Hess PJ Jr, Klodell CT, Ejaz AA et al. RIFLE criteria for acute kidney injury in aortic arch surgery. J Thorac Cardiovasc Surg 2007;134:1554–60. - PubMed
-
- Englberger L, Suri RM, Greason KL, Burkhart HM, Sundt TM, Daly RC et al. Deep hypothermic circulatory arrest is not a risk factor for acute kidney injury in thoracic aortic surgery. J Thorac Cardiovasc Surg 2011;141:552–8. - PubMed
-
- Kim WH, Lee SM, Choi JW, Kim EH, Lee JH, Jung JW et al. Simplified clinical risk score to predict acute kidney injury after aortic surgery. J Cardiothorac Vasc Anesth 2013;27:1158–66. - PubMed
-
- Pacini D, Pantaleo A, Di Marco L, Leone A, Barberio G, Parolari A et al. Risk factors for acute kidney injury after surgery of the thoracic aorta using antegrade selective cerebral perfusion and moderate hypothermia. J Thorac Cardiovasc Surg 2015;150:127–33.e1. - PubMed
-
- Ghincea C, Reece TB, Eldeiry M, Roda GF, Bronsert MR, Jarrett MJ et al. Predictors of acute kidney injury following aortic arch surgery. J Surg Res 2019;242:40–6. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
