

Association of autosomal dominant polycystic kidney disease with cerebral small vessel disease
- PMID: 34415212
- PMCID: PMC8669289
- DOI: 10.1177/0271678X211037869
Association of autosomal dominant polycystic kidney disease with cerebral small vessel disease
Abstract
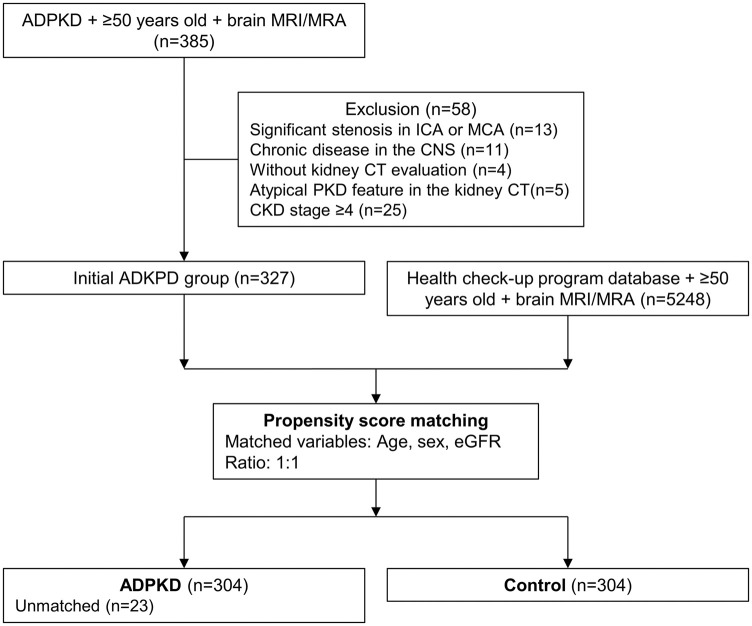
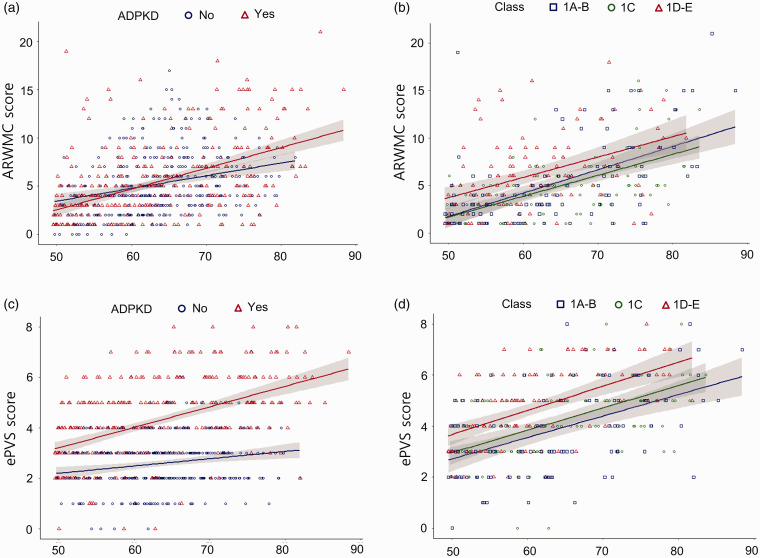
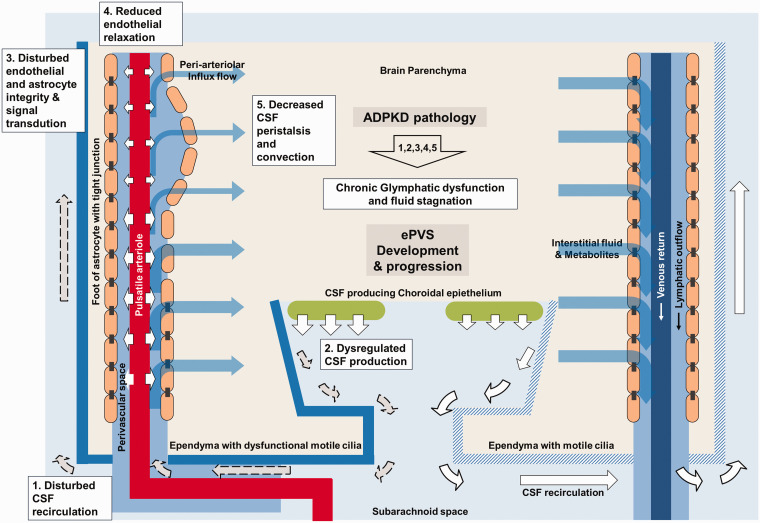
Cilia dysfunction in autosomal-dominant polycystic kidney disease (ADPKD) may impair the integrity of glymphatic system and be implicated in the progression of cerebral small vessel disease (SVD), although the link between the two diseases has not been investigated. We evaluated the association of ADPKD pathology with SVD pattern and severity. Overall, 304 individuals in an ADPKD (chronic kidney disease stage ≤4 and age ≥50 years) cohort and their age, sex, and estimated glomerular filtration rate (eGFR)-matched controls were retrospectively included. ADPKD severity was classified into 1 A-B, 1 C, and 1 D-E, according to age and height-adjusted total kidney volume. SVD parameters included white-matter hyperintensity (WMH) severity scale, enlarged perivascular space (ePVS) score, and degree of lacunes or cerebral microbleeds (CMBs). After adjustments for age, sex, eGFR, and cerebrovascular risk factor parameters, ADPKD was associated with higher ePVS scores (P < 0.001), but not with the WMH severity or degree of lacunes or CMBs. In the ADPKD subgroup, higher ADPKD severity class was associated with higher ePVS scores (P < 0.001), WMH severity (P = 0.003), and degree of lacunes (P = 0.002). ADPKD associated cilia dysfunction may induce chronic cerebral glymphatic system dysfunction, which may contribute to the specific progression of ePVS compared with other SVD markers.
Keywords: Autosomal dominant polycystic kidney disease; cilia dysfunction; enlarged perivascular space; glymphatic system; small vessel disease.
Conflict of interest statement
Figures
References
-
- Yoshida H, Higashihara E, Maruyama K, et al. Relationship between intracranial aneurysms and the severity of autosomal dominant polycystic kidney disease. Acta Neurochir (Wien) 2017; 159: 2325–2330. - PubMed
-
- Schievink WI, Torres VE, Wiebers DO, et al. Intracranial arterial dolichoectasia in autosomal dominant polycystic kidney disease. J Am Soc Nephrol 1997; 8: 1298–1303. - PubMed
-
- Wang D, Iversen J, Wilcox CS, et al. Endothelial dysfunction and reduced nitric oxide in resistance arteries in autosomal-dominant polycystic kidney disease. Kidney Int 2003; 64: 1381–1388. - PubMed
-
- Chapman AB, Johnson A, Gabow PA, et al. The renin–angiotensin–aldosterone system and autosomal dominant polycystic kidney disease. N Engl J Med 1990; 323: 1091–1096. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
