

Long-term glucocorticoid treatment and high relapse rate remain unresolved issues in the real-life management of polymyalgia rheumatica: a systematic literature review and meta-analysis
- PMID: 34415462
- PMCID: PMC8724087
- DOI: 10.1007/s10067-021-05819-z
Long-term glucocorticoid treatment and high relapse rate remain unresolved issues in the real-life management of polymyalgia rheumatica: a systematic literature review and meta-analysis
Abstract
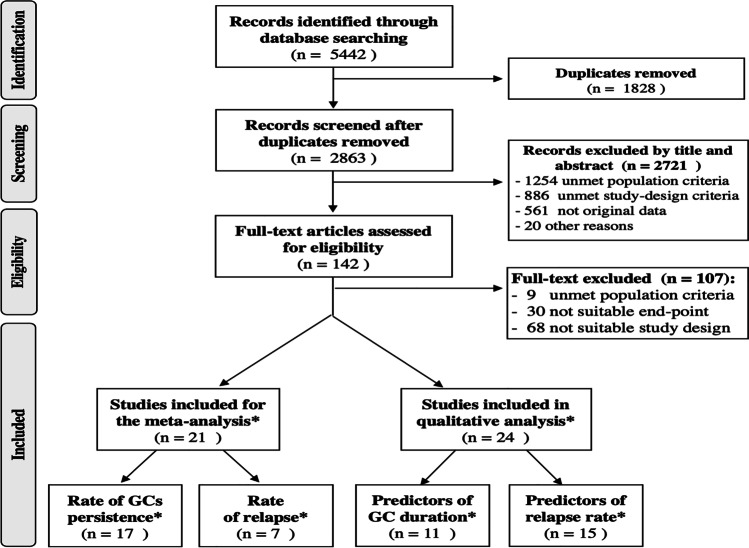
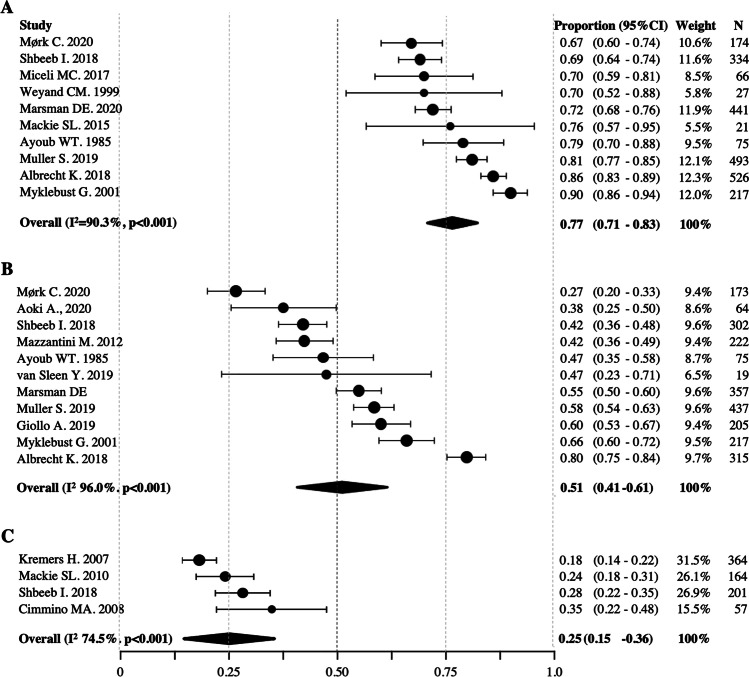
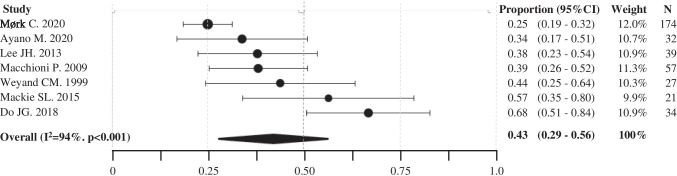
A systematic review and meta-analysis were conducted, according to the PRISMA methodology, to summarize current evidence on the prevalence and predictors of long-term glucocorticoid (GC) treatment and disease relapses in the real-life management of polymyalgia rheumatica (PMR).Out of 5442 retrieved studies, 21 were eligible for meta-analysis and 24 for qualitative analysis. The pooled proportions of patients still taking GCs at 1, 2, and 5 years were respectively 77% (95%CI 71-83%), 51% (95%CI 41-61%), and 25% (95CI% 15-36%). No significant difference was recorded by distinguishing study cohorts recruited before and after the issue of the international recommendations in 2010. The pooled proportion of patients experiencing at least one relapse at 1 year from treatment initiation was 43% (95%CI 29-56%). Female gender, acute-phase reactants levels, peripheral arthritis, starting GCs dosage, and tapering speed were the most frequently investigated potential predictors of prolonged GC treatment and relapse, but with inconsistent results. Only a few studies and with conflicting results evaluated the potential role of early treatment with methotrexate in reducing the GC exposure and the risk of relapse in PMR.This study showed that a high rate of prolonged GC treatment is still recorded in the management of PMR. The relapse rate, even remarkable, can only partially explain the long-term GC treatment, suggesting that other and not yet identified factors may be involved. Additional research is needed to profile patients with a higher risk of long-term GC treatment and relapse and identify more effective steroid-sparing strategies. Key Points: • High rate of long-term glucocorticoid (GC) treatment is recorded in polymyalgia rheumatica (PMR), being 77%, 51%, and 25% of patients still on GCs after respectively 1, 2, and 5 years. • A pooled relapse rate of 43% at 1 year, even remarkable, can only partially explain the long-term GC treatment in PMR. • Several studies have attempted to identify potential predictors of prolonged treatment with GCs and relapse, but with inconsistent results. • Additional research is needed to profile patients with a higher risk of long-term GC treatment and relapse and identify more effective steroid-sparing strategies.
Keywords: Glucocorticoids; Meta-analysis; Observational study; Polymyalgia rheumatica; Relapse.
© 2021. The Author(s).
Figures
Comment in
-
Long-term glucocorticoid treatment in patients with polymyalgia rheumatica: can we just move a step forward? Comments on "Long-term glucocorticoid treatment and high relapse rate remain unresolved issues in the real-life management of polymyalgia rheumatica: a systematic literature review and meta-analysis".Clin Rheumatol. 2021 Oct;40(10):4367-4368. doi: 10.1007/s10067-021-05898-y. Epub 2021 Aug 30. Clin Rheumatol. 2021. PMID: 34460020 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
