

Preterm births in China between 2012 and 2018: an observational study of more than 9 million women
- PMID: 34416213
- PMCID: PMC8386289
- DOI: 10.1016/S2214-109X(21)00298-9
Preterm births in China between 2012 and 2018: an observational study of more than 9 million women
Abstract
Background: Preterm birth rates have increased significantly worldwide over the past decade. Few epidemiological studies on the incidence of preterm birth and temporal trends are available in China. This study used national monitoring data from China's National Maternal Near Miss Surveillance System (NMNMSS) to estimate the rate of preterm birth and trends between 2012 and 2018 in China and to assess risk factors associated with preterm birth.
Methods: In this observational study, data were sourced from the NMNMSS between Jan 1, 2012, and Dec 31, 2018. Pregnancies with at least one livebirth, with the baby born at 28 weeks of gestation or more or 1000 g or more birthweight were included. We estimated the rates of overall preterm, very preterm (born between 28 and 31 weeks' gestation), moderate preterm (born between 32 and 33 weeks' gestation), and late preterm (born between 34 and 36 weeks' gestation) births in singleton and multiple pregnancies and assessed their trends over time. We used logistic regression analysis to examine the associations between preterm birth and sociodemographic characteristics and obstetric complications, considering the sampling strategy and clustering of births within hospitals. Interrupted time series analysis was used to assess the changes in preterm birth rates during the period of the universal two child policy intervention.
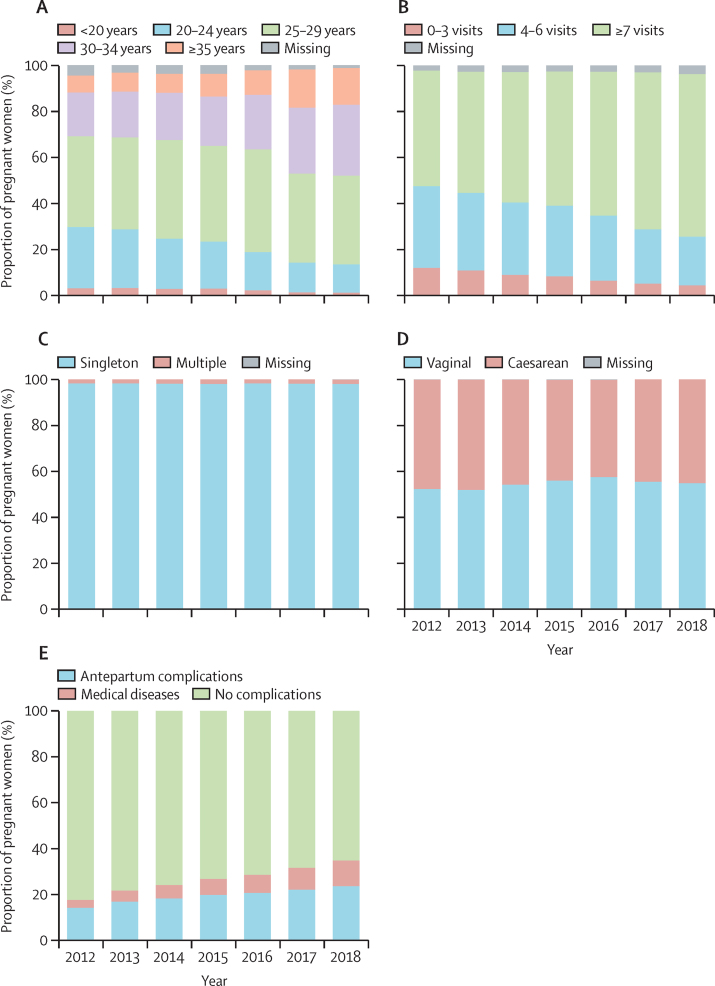
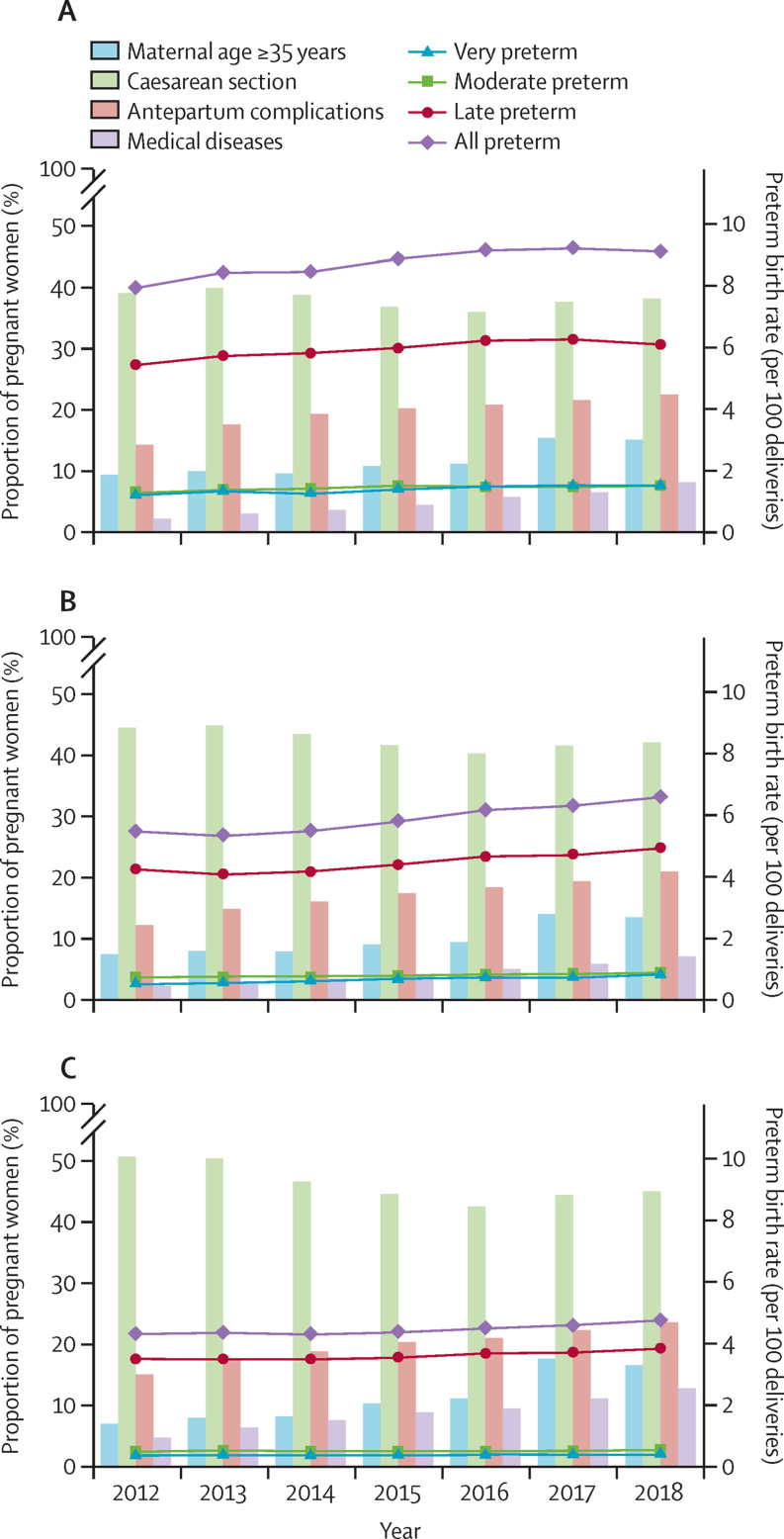
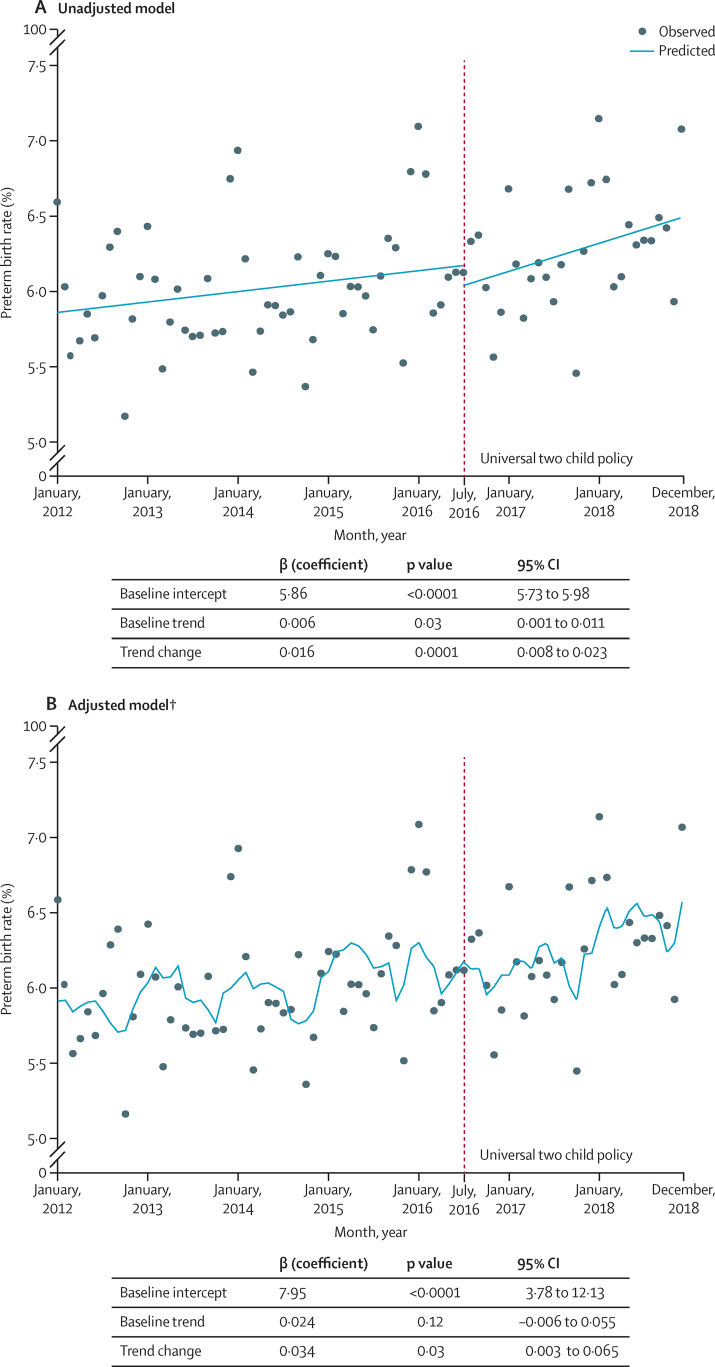
Findings: From Jan 1, 2012, to Dec 31, 2018, 9 645 646 women gave birth to at least one live baby, of whom 665 244 (6·1%) were born preterm. In all pregnancies, the overall preterm birth rate increased from 5·9% in 2012 to 6·4% in 2018 (8·8% increase; annual rate of increase [ARI] 1·3 [95% CI 0·6 to 2·1]). Late preterm births (8·8%; ARI 1·5% [0·9 to 2·2]) and very preterm births (13·3%; ARI 1·8% [0·5 to 3·0]) significantly increased from 2012 to 2018, whereas moderate preterm births did not (3·8%; ARI 0·3% [95% CI -0·9 to 1·5]). In singleton pregnancies, the overall preterm birth rate showed a small but significant 6·4% increase (ARI 1·0% [0·4 to 1·7]) over the 7 year period. In multiple pregnancies, the overall preterm birth rate significantly increased from 46·8% in 2012 to 52·7% in 2018 (12·4% increase; ARI 1·9% [1·2 to 2·6]). Compared with women who gave birth in 2012, those who gave birth in 2018 were more likely to be older (aged ≥35 years; 7·4% in 2012 vs 15·9% in 2018), have multiples (1·6% vs 1·9%), have seven or more antenatal visits (50·2% vs 70·7%), and have antepartum complications and medical disease (17·9% vs 35·1%), but they were less likely to deliver via caesarean section (47·5% vs 45·0%). Compared with the baseline period (January, 2012 to June, 2016), a higher increase in preterm birth was observed after the universal two child policy came into effect in July, 2016 (β=0·034; p=0·03).
Interpretation: An increase in preterm births was noted for both singleton and multiple pregnancies between 2012 and 2018 in China. China's strategic investment in maternal and neonatal health has been crucial for the prevention of preterm birth. Due to rapid changes in sociodemographic and obstetric factors related to preterm birth-particularly within the context of the universal two child policy-such as advanced maternal age at delivery, maternal complications, and multiple pregnancies, greater efforts to reduce the burden of preterm birth are urgently needed.
Funding: National Key R&D Program of China, National Health Commission of the People's Republic of China, China Medical Board, WHO, and UNICEF.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Comment in
-
The rising preterm birth rate in China: a cause for concern.Lancet Glob Health. 2021 Sep;9(9):e1179-e1180. doi: 10.1016/S2214-109X(21)00337-5. Lancet Glob Health. 2021. PMID: 34416201 No abstract available.
References
-
- Moster D, Lie RT, Markestad T. Long-term medical and social consequences of preterm birth. NEJM. 2008;359:262–273. - PubMed
-
- Saigal S, Doyle LW. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet. 2008;371:261–269. - PubMed
-
- Vogel JP, Chawanpaiboon S, Moller AB, Watananirun K, Bonet M, Lumbiganon P. The global epidemiology of preterm birth. Best Pract Res Clin Obstet Gynaecol. 2018;52:3–12. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
