

Failure of OPHL type IIb due to undiagnosed Eagle syndrome
- PMID: 34417247
- PMCID: PMC8381297
- DOI: 10.1136/bcr-2021-244589
Failure of OPHL type IIb due to undiagnosed Eagle syndrome
Abstract
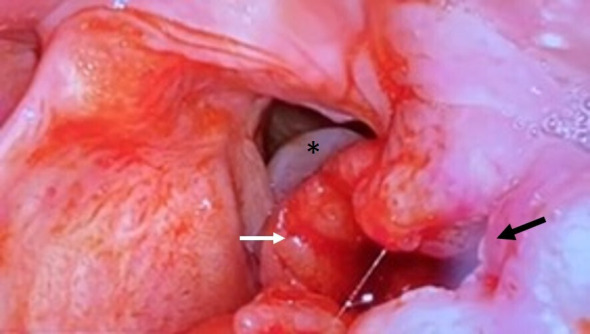
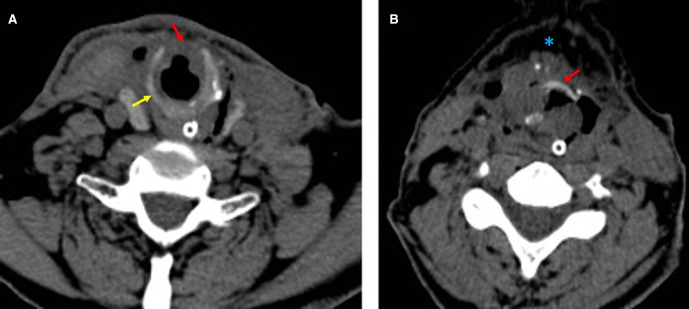
A 52-year-old man with glottic-supraglottic tumour underwent open partial horizontal laryngectomy (OPHL) IIb. On the 12th day postoperative, laryngoscopy showed necrotic tissue at the level of pexy and an increased distance between tongue base and neoglottis; the neck CT showed cricoid arch rupture and rupture of the pexy. By re-examining the preoperative CT images, the ossification of stylohyoid ligament (Eagle syndrome) was detected and supposed as the possible cause of cricoid rupture due to its traction on the hyoid bone and therefore on the pexy. The stylohyoid ligaments were cut at their insertion on the hyoid bone and a tracheohyoidopexy was performed. Two months after surgery, the patient had only some swallowing impairments. This case represents a complication in OPHL II never reported in literature caused by an undiagnosed Eagle syndrome in preoperative, pointing out the importance to search for any anatomical anomaly that could jeopardise the success of the surgery.
Keywords: cancer intervention; ear; head and neck cancer; head and neck surgery; nose and throat/otolaryngology; radiology.
© BMJ Publishing Group Limited 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


Similar articles
-
[Re-evaluation of 191 larynx cancer surgeries according to the Open Partial Horizontal Laryngectomies classification proposed by European Laryngological Society working committee in 2014].Otolaryngol Pol. 2014 Nov-Dec;68(6):281-6. doi: 10.1016/j.otpol.2014.07.001. Epub 2014 Jul 31. Otolaryngol Pol. 2014. PMID: 25152380 Polish.
-
Eagle syndrome: elongated stylohyoid-associated facial pain.BMJ Case Rep. 2020 Mar 24;13(3):e234024. doi: 10.1136/bcr-2019-234024. BMJ Case Rep. 2020. PMID: 32209578 Free PMC article. No abstract available.
-
Eagle syndrome compared with stylohyoid syndrome: complete ossification of the stylohyoid ligament and joint.Br J Oral Maxillofac Surg. 2017 Feb;55(2):218-219. doi: 10.1016/j.bjoms.2016.07.002. Epub 2016 Jul 18. Br J Oral Maxillofac Surg. 2017. PMID: 27435498 No abstract available.
-
Eagle and Ernest syndromes: a scoping review.Minerva Dent Oral Sci. 2024 Apr;73(2):119-130. doi: 10.23736/S2724-6329.22.04724-6. Epub 2022 Oct 5. Minerva Dent Oral Sci. 2024. PMID: 36197280
-
Treatment of Eagle syndrome with transcervical approach secondary to a failed intraoral attempt: Surgical technique and literature review.J Stomatol Oral Maxillofac Surg. 2017 Dec;118(6):353-358. doi: 10.1016/j.jormas.2017.06.017. Epub 2017 Jul 10. J Stomatol Oral Maxillofac Surg. 2017. PMID: 28705777 Review.
References
-
- HOFMANN-SAGUEZ R. [Conservative subtotal laryngectomy]. Ann Otolaryngol 1950;67:811–6. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources