

Burn Resuscitation Practices in North America: Results of the Acute Burn ResUscitation Multicenter Prospective Trial (ABRUPT)
- PMID: 34417368
- PMCID: PMC8857312
- DOI: 10.1097/SLA.0000000000005166
Burn Resuscitation Practices in North America: Results of the Acute Burn ResUscitation Multicenter Prospective Trial (ABRUPT)
Abstract
Objectives: ABRUPT was a prospective, noninterventional, observational study of resuscitation practices at 21 burn centers. The primary goal was to examine burn resuscitation with albumin or crystalloids alone, to design a future prospective randomized trial.
Summary background data: No modern prospective study has determined whether to use colloids or crystalloids for acute burn resuscitation.
Methods: Patients ≥18 years with burns ≥ 20% total body surface area (TBSA) had hourly documentation of resuscitation parameters for 48 hours. Patients received either crystalloids alone or had albumin supplemented to crystalloid based on center protocols.
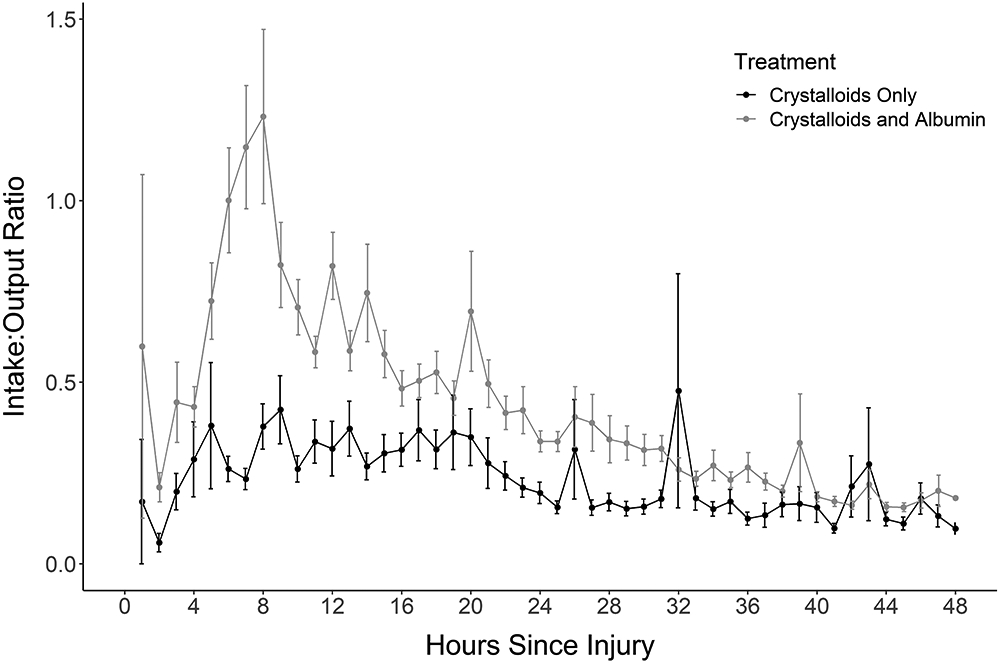
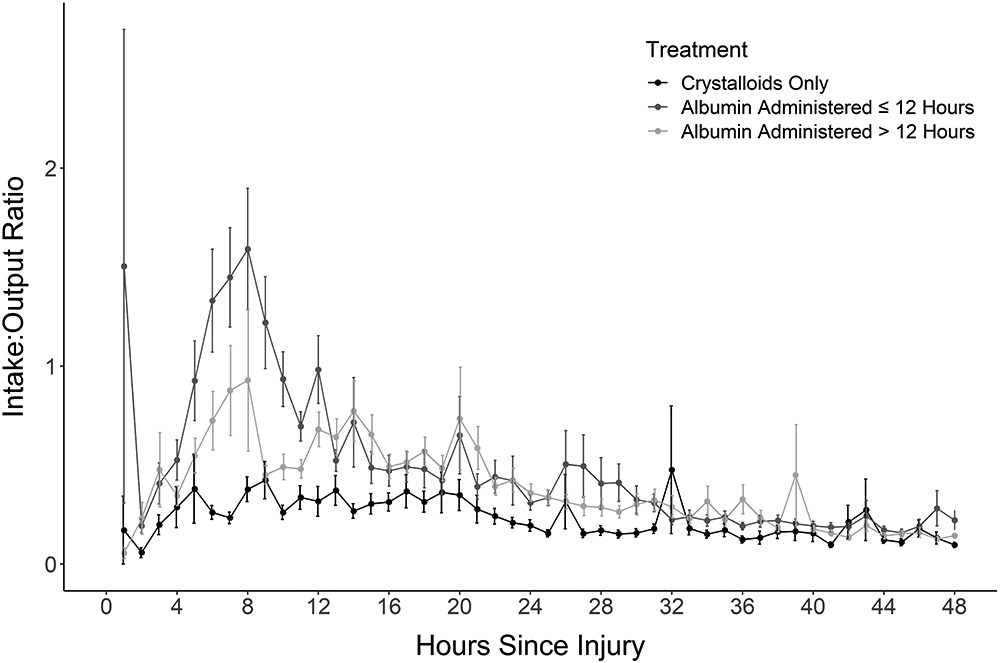
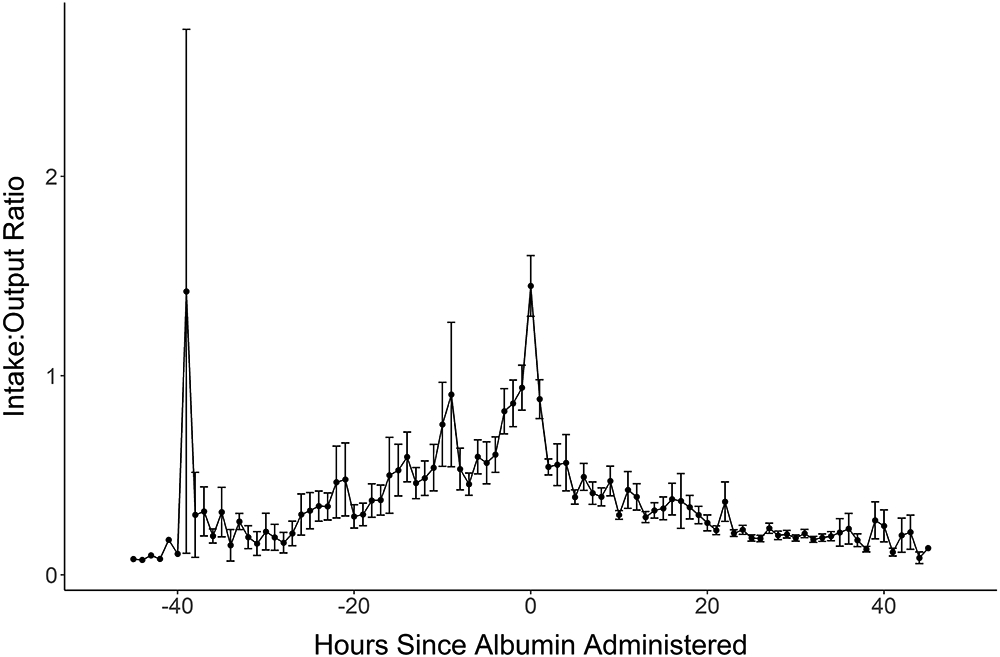
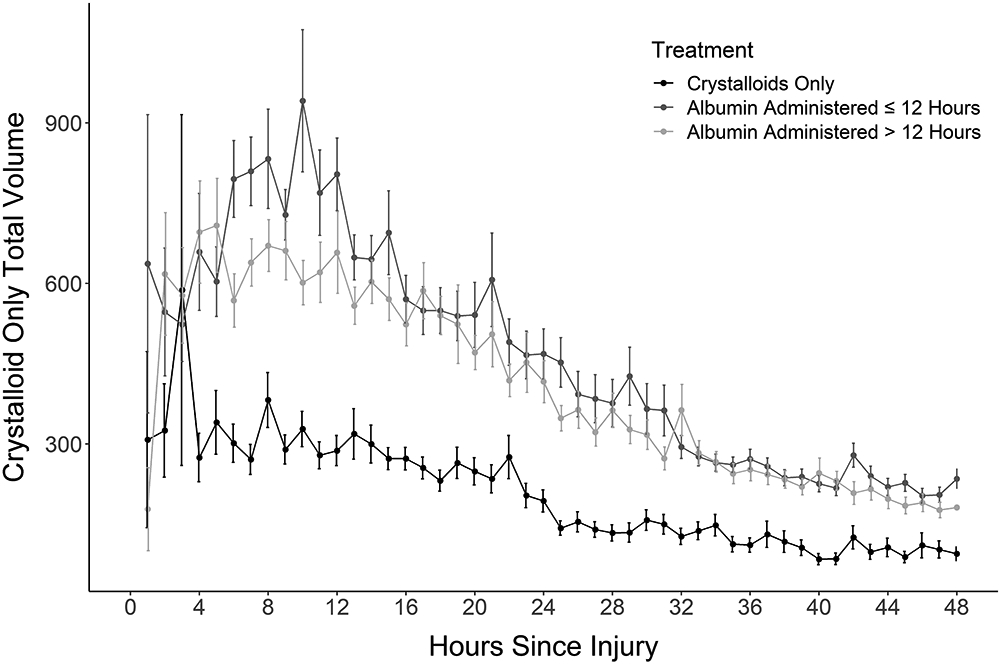
Results: Of 379 enrollees, two-thirds (253) were resuscitated with albumin and one-third (126) were resuscitated with crystalloid alone. Albumin patients received more total fluid than Crystalloid patients (5.2 ± 2.3 vs 3.7 ± 1.7 mL/kg/% TBSA burn/24 hours), but patients in the Albumin Group were older, had larger burns, higher admission Sequential Organ Failure Assessment (SOFA) scores, and more inhalation injury. Albumin lowered the in-to-out (I/O) ratio and was started ≤12 hours in patients with the highest initial fluid requirements, given >12 hours with intermediate requirements, and avoided in patients who responded to crystalloid alone.
Conclusions: Albumin use is associated with older age, larger and deeper burns, and more severe organ dysfunction at presentation. Albumin supplementation is started when initial crystalloid rates are above expected targets and improves the I/O ratio. The fluid received in the first 24 hours was at or above the Parkland Formula estimate.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
ABRUPT Financial Disclosures: Conflict of Interest: A.G.: Consultant for Mallinckrodt, Inc.; L.A.W.: Research support from Avita, Inc., MEDIWound, Inc., Mallincrodt, Inc.; J.H.H.: Equity in Abbott Labs, AbbVie, Change Healthcare, Imbed Biosciences, and consultant for Avita, Inc. and Mallinckrodt, Inc.; K.N.F.: Consultant for Baxter, Integra, Inc., Skingenix; A.K.: Consultant for Avita, Inc. The authors report no conflicts of interest.
Figures
References
-
- Baxter CR, Shires T. Physiological response to crystalloid resuscitation of severe burns. Ann N Y Acad Sci 1968;150:874–94. - PubMed
-
- Baxter CR, Marvin J, Curreri PW. Fluid and electrolyte therapy of burn shock. Heart Lung 1973;2:707–13. - PubMed
-
- Pruitt BA Jr. Protection from excessive resuscitation: pushing the pendulum back. J Trauma 2000;49:567–568. - PubMed
-
- Saffle JR. The phenomenon of “fluid creep” in acute burn resuscitation. J Burn Care and Res 2007;28:382–95. - PubMed
-
- Cartotto R, Zhou A. Fluid Creep: The Pendulum Hasn’t Swung Back Yet! J Burn Care and Res 2010; 31:551–559. - PubMed
