

Investigation of spleen CXCR4 expression by [68Ga]Pentixafor PET in a cohort of 145 solid cancer patients
- PMID: 34417915
- PMCID: PMC8380222
- DOI: 10.1186/s13550-021-00822-6
Investigation of spleen CXCR4 expression by [68Ga]Pentixafor PET in a cohort of 145 solid cancer patients
Abstract
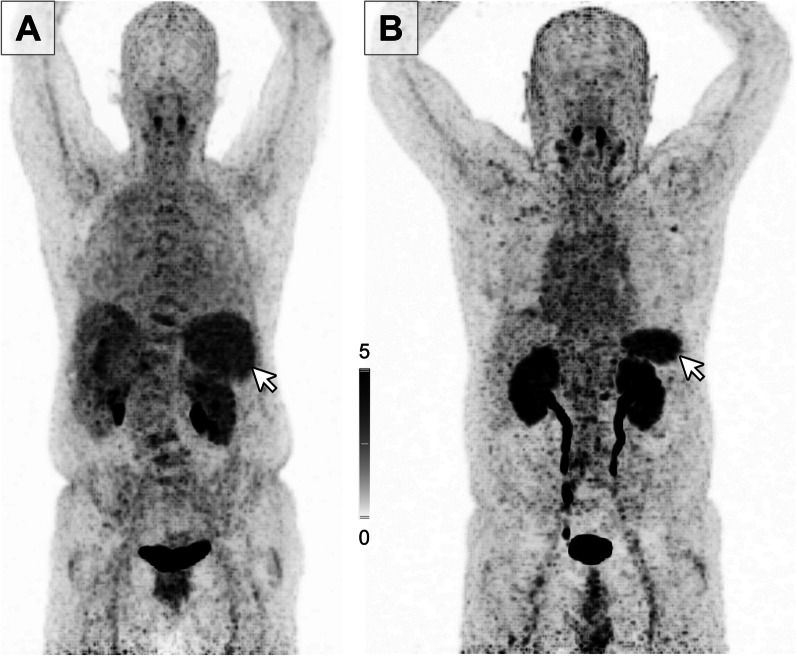
Background: The chemokine receptor CXCR4 is frequently overexpressed and associated with adverse prognosis in most hematopoietic malignancies and solid cancers. Recently, CXCR4 molecular imaging using the CXCR4-specific positron emission tomography (PET) tracer Pentixafor ([68Ga]Pentixafor) has become a well-established method to non-invasively measure CXCR4 expression in vivo. In previous Pentixafor imaging studies, highly variable CXCR4 tracer uptake to the spleen was observed.
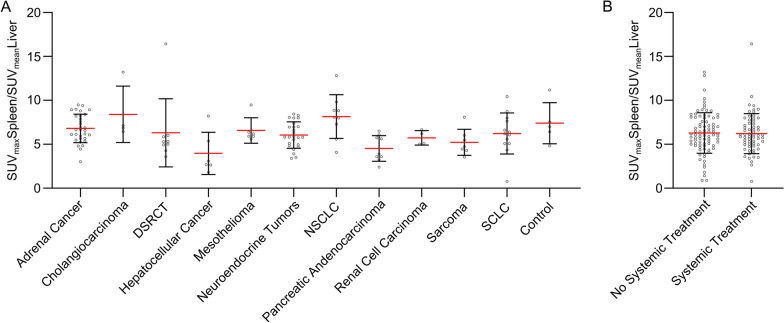
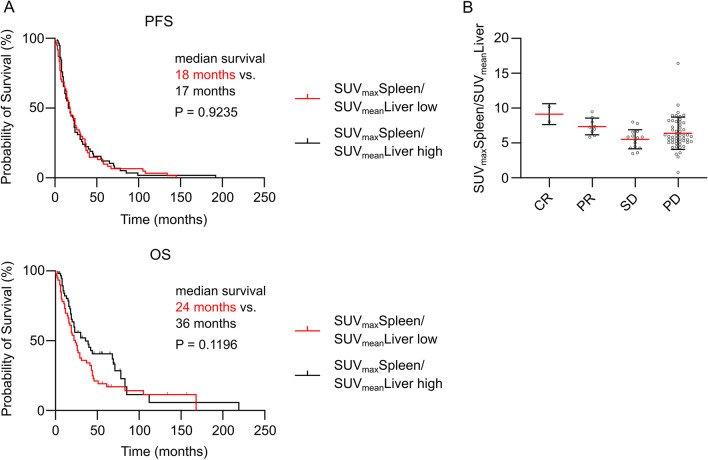
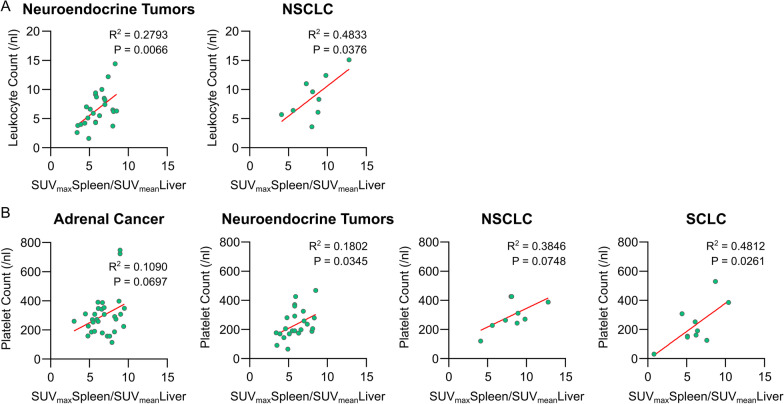
Results: We investigated the hypothesis that enhanced spleen [68Ga]Pentixafor uptake and thus CXCR4 expression in patients with solid tumors would indicate an activated spleen state and/or an association with clinical and prognostic features and survival parameters. In this retrospective study, [68Ga]Pentixafor-PET images and patient records of 145 solid tumor patients representing 27 cancer entities were investigated for an association of spleen [68Ga]Pentixafor uptake and clinical characteristics and outcome. Based on this assessment, we did not observe differences in clinical outcomes, measured by progression-free survival, overall survival and remission status neither within the entire cohort nor within subgroups of adrenal cancer, desmoplastic small round cell tumor, neuroendocrine tumors, non-small cell lung cancer, small cell lung cancer and pancreatic adenocarcinoma patients. No tumor entity showed especially high levels of spleen [68Ga]Pentixafor uptake compared to others or a control cohort. However, when investigating laboratory parameters, there was a positive correlation of high spleen [68Ga]Pentixafor uptake with leukocyte and/or platelet counts in neuroendocrine tumors, non-small cell lung cancer and small cell lung cancer.
Conclusion: Spleen [68Ga]Pentixafor uptake was not associated with stage of disease and clinical outcomes in solid tumor patients. We identified positively associated platelet and/or leukocyte counts with spleen [68Ga]Pentixafor uptake in neuroendocrine tumors, non-small cell lung cancer and small cell lung cancer, suggesting that splenic CXCR4 expression could possibly play a role in systemic immunity/inflammation in some types of solid tumors or a subgroup of patients within solid tumor entities.
Keywords: CXCR4; Clinical studies; Molecular imaging; PET; Pentixafor; Retrospective studies; Solid tumors; Spleen; Uptake.
© 2021. The Author(s).
Conflict of interest statement
U.K. has served on the advisory board of PentixaPharm, the company that is developing clinical applications for Pentixafor and Pentixather. H.-J.W. is a founder, shareholder and advisory board member of Scintomics GmbH, Fürstenfeldbruck, Germany.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
