

Plasma phosphorylated tau 217 and phosphorylated tau 181 as biomarkers in Alzheimer's disease and frontotemporal lobar degeneration: a retrospective diagnostic performance study
- PMID: 34418401
- PMCID: PMC8711249
- DOI: 10.1016/S1474-4422(21)00214-3
Plasma phosphorylated tau 217 and phosphorylated tau 181 as biomarkers in Alzheimer's disease and frontotemporal lobar degeneration: a retrospective diagnostic performance study
Erratum in
-
Correction to Lancet Neurol 2021; 20: 739-52.Lancet Neurol. 2021 Oct;20(10):e6. doi: 10.1016/S1474-4422(21)00286-6. Epub 2021 Aug 31. Lancet Neurol. 2021. PMID: 34478638 No abstract available.
Abstract
Background: Plasma tau phosphorylated at threonine 217 (p-tau217) and plasma tau phosphorylated at threonine 181 (p-tau181) are associated with Alzheimer's disease tau pathology. We compared the diagnostic value of both biomarkers in cognitively unimpaired participants and patients with a clinical diagnosis of mild cognitive impairment, Alzheimer's disease syndromes, or frontotemporal lobar degeneration (FTLD) syndromes.
Methods: In this retrospective multicohort diagnostic performance study, we analysed plasma samples, obtained from patients aged 18-99 years old who had been diagnosed with Alzheimer's disease syndromes (Alzheimer's disease dementia, logopenic variant primary progressive aphasia, or posterior cortical atrophy), FTLD syndromes (corticobasal syndrome, progressive supranuclear palsy, behavioural variant frontotemporal dementia, non-fluent variant primary progressive aphasia, or semantic variant primary progressive aphasia), or mild cognitive impairment; the participants were from the University of California San Francisco (UCSF) Memory and Aging Center, San Francisco, CA, USA, and the Advancing Research and Treatment for Frontotemporal Lobar Degeneration Consortium (ARTFL; 17 sites in the USA and two in Canada). Participants from both cohorts were carefully characterised, including assessments of CSF p-tau181, amyloid-PET or tau-PET (or both), and clinical and cognitive evaluations. Plasma p-tau181 and p-tau217 were measured using electrochemiluminescence-based assays, which differed only in the biotinylated antibody epitope specificity. Receiver operating characteristic analyses were used to determine diagnostic accuracy of both plasma markers using clinical diagnosis, neuropathological findings, and amyloid-PET and tau-PET measures as gold standards. Difference between two area under the curve (AUC) analyses were tested with the Delong test.
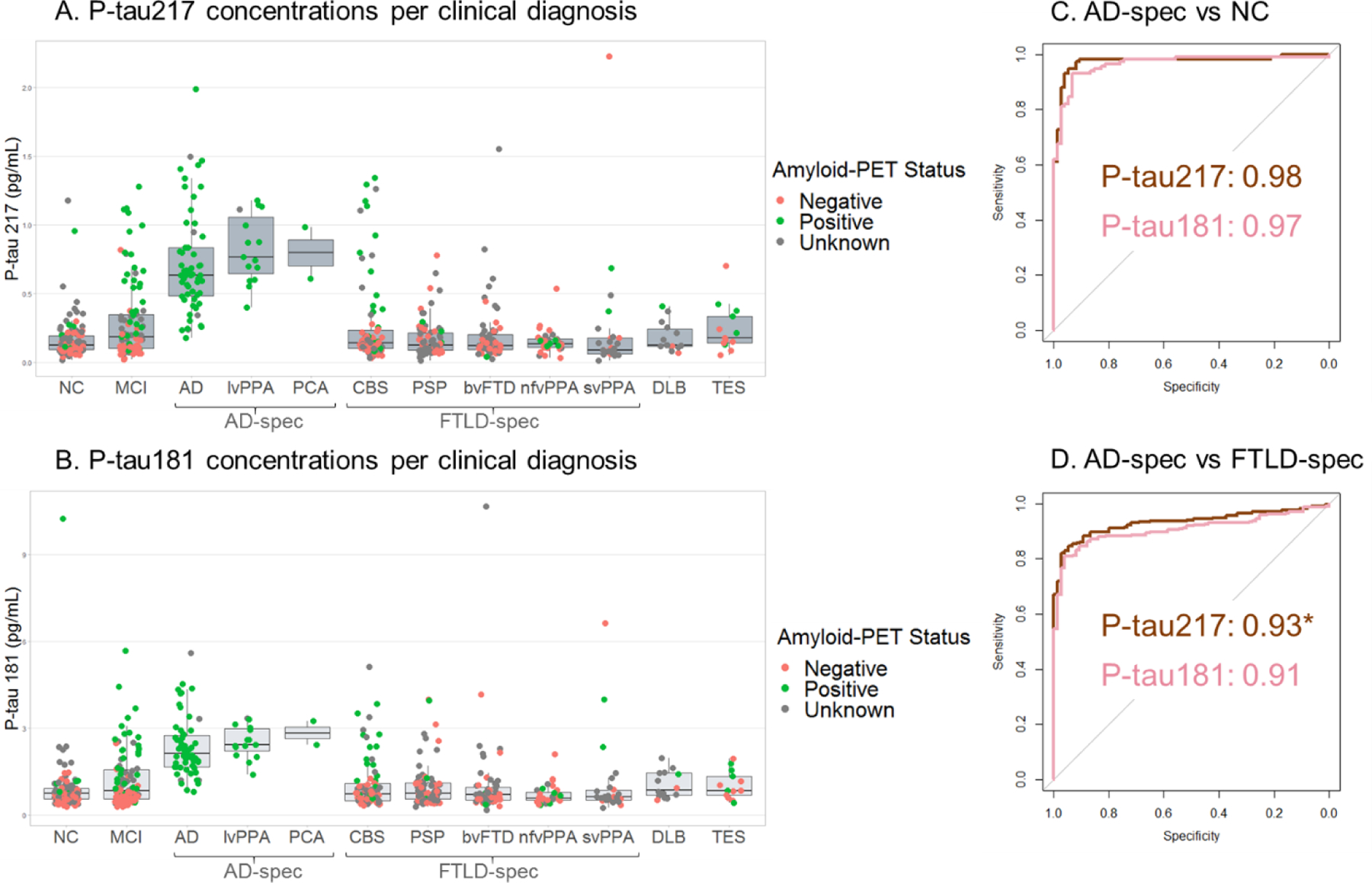
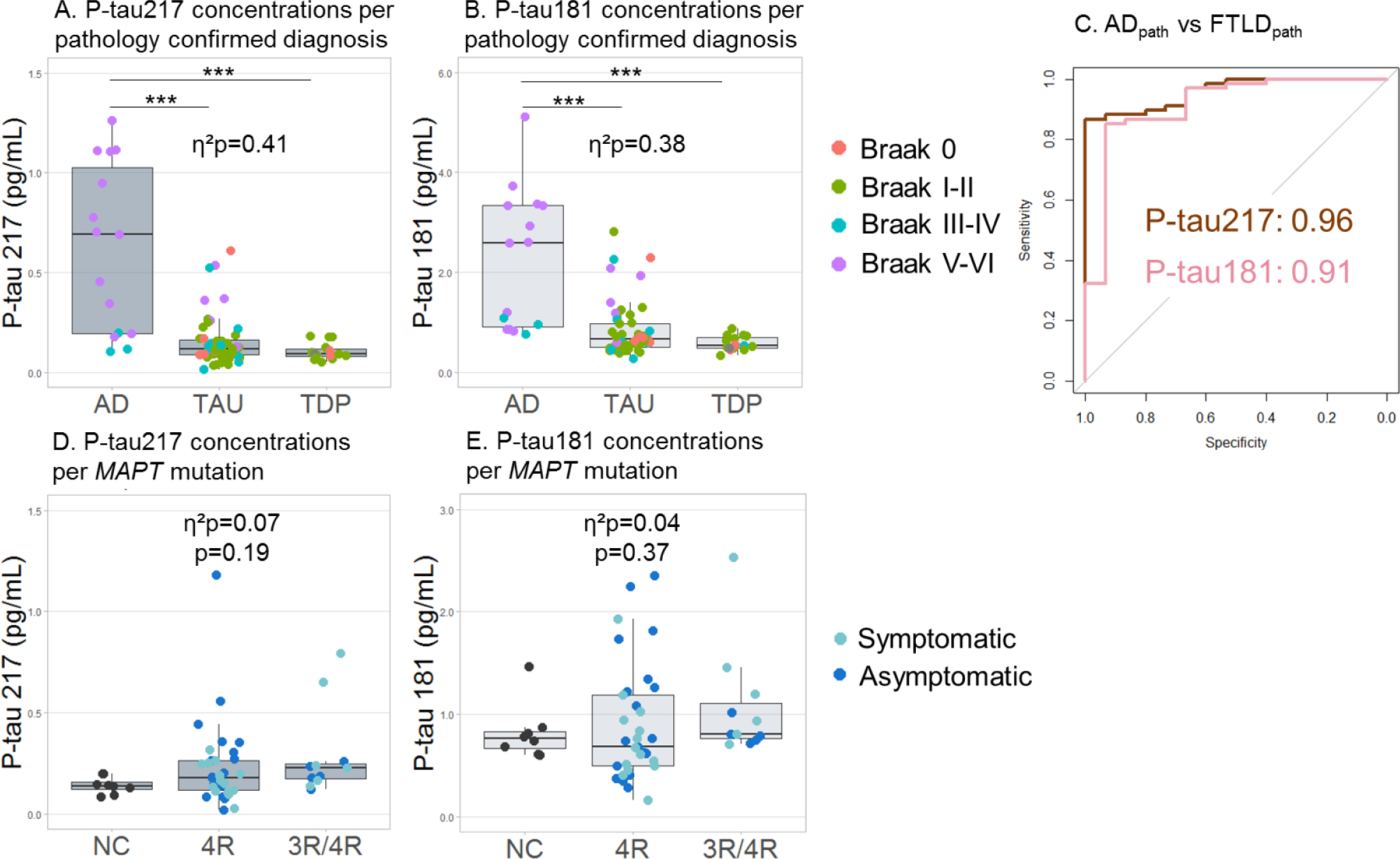
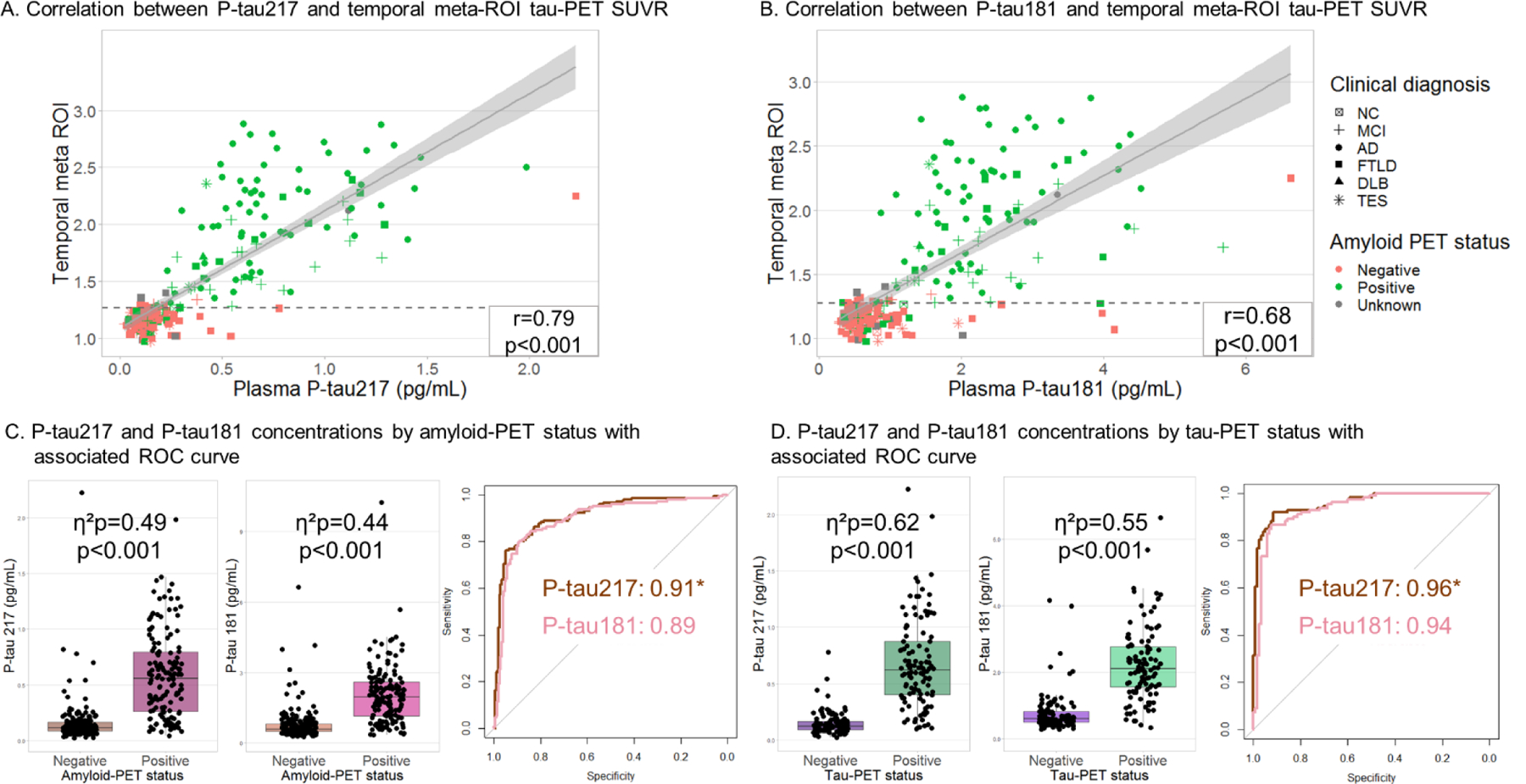
Findings: Data were collected from 593 participants (443 from UCSF and 150 from ARTFL, mean age 64 years [SD 13], 294 [50%] women) between July 1 and Nov 30, 2020. Plasma p-tau217 and p-tau181 were correlated (r=0·90, p<0·0001). Both p-tau217 and p-tau181 concentrations were increased in people with Alzheimer's disease syndromes (n=75, mean age 65 years [SD 10]) relative to cognitively unimpaired controls (n=118, mean age 61 years [SD 18]; AUC=0·98 [95% CI 0·95-1·00] for p-tau217, AUC=0·97 [0·94-0·99] for p-tau181; pdiff=0·31) and in pathology-confirmed Alzheimer's disease (n=15, mean age 73 years [SD 12]) versus pathologically confirmed FTLD (n=68, mean age 67 years [SD 8]; AUC=0·96 [0·92-1·00] for p-tau217, AUC=0·91 [0·82-1·00] for p-tau181; pdiff=0·22). P-tau217 outperformed p-tau181 in differentiating patients with Alzheimer's disease syndromes (n=75) from those with FTLD syndromes (n=274, mean age 67 years [SD 9]; AUC=0·93 [0·91-0·96] for p-tau217, AUC=0·91 [0·88-0·94] for p-tau181; pdiff=0·01). P-tau217 was a stronger indicator of amyloid-PET positivity (n=146, AUC=0·91 [0·88-0·94]) than was p-tau181 (n=214, AUC=0·89 [0·86-0·93]; pdiff=0·049). Tau-PET binding in the temporal cortex was more strongly associated with p-tau217 than p-tau181 (r=0·80 vs r=0·72; pdiff<0·0001, n=230).
Interpretation: Both p-tau217 and p-tau181 had excellent diagnostic performance for differentiating patients with Alzheimer's disease syndromes from other neurodegenerative disorders. There was some evidence in favour of p-tau217 compared with p-tau181 for differential diagnosis of Alzheimer's disease syndromes versus FTLD syndromes, as an indication of amyloid-PET-positivity, and for stronger correlations with tau-PET signal. Pending replication in independent, diverse, and older cohorts, plasma p-tau217 and p-tau181 could be useful screening tools to identify individuals with underlying amyloid and Alzheimer's disease tau pathology.
Funding: US National Institutes of Health, State of California Department of Health Services, Rainwater Charitable Foundation, Michael J Fox foundation, Association for Frontotemporal Degeneration, Alzheimer's Association.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests JLD and NKP are employees of Eli Lilly and Company, which is exploring commercial development opportunities for p-tau assays. JLD is listed as an inventor on a patent related to reagents used in the p-tau assays. HZ has served at scientific advisory boards for Denali, Roche Diagnostics, Wave, Samumed, Siemens Healthineers, Pinteon Therapeutics, and CogRx, has given lectures in symposia sponsored by Fujirebio, Alzecure, and Biogen, and is a cofounder of Brain Biomarker Solutions (BBS) in Gothenburg AB, which is a part of the GU Ventures Incubator Program. OH has acquired research support (for the institution) from AVID Radiopharmaceuticals, Biogen, Eli Lilly, Eisai, GE Healthcare, Pfizer, and Roche. In the past 2 years, he has received consultancy or speaker fees from AC Immune, Alzpath, Biogen, Cerveau, and Roche. KB served as a consultant, at advisory boards, or at data monitoring committees for Abcam, Axon, Biogen, JOMDD/Shimadzu, Julius Clinical, Lilly, MagQu, Novartis, Roche Diagnostics, and Siemens Healthineers, and is a cofounder of BBS in Gothenburg AB, outside the submitted work. LTG receives research support from Avid Radiopharmaceuticals and Eli Lilly. She has received consulting fees from the Simon Foundation and Cura Sen, and serves as associate editor for Frontiers in Aging Neurosciences, Frontiers in Dementia, and the Journal of Alzheimer Disease. HR has received research support from Biogen Pharmaceuticals, has consulting agreements with Wave Neuroscience and Ionis Pharmaceuticals, and receives research support from US National Institutes of Health (NIH). BFB receives research support from NIH, the Mangurian Foundation, and the Little Family Foundation. He is on the Scientific Advisory Board for the Tau Consortium, and has received grant support for clinical trials from Biogen, Alector, and EIP Pharma. GDR receives research support from NIH, Alzheimer's Association, American College of Radiology, Rainwater Charitable Foundation, Avid Radiopharmaceuticals, Eli Lilly, GE Healthcare, and Life Molecular Imaging. He has served as a consultant for Eisai, Merck, Axon Neurosciences, and Johnson & Johnson, and has received speaking honoraria from GE Healthcare. He serves as Associate Editor for JAMA Neurology. JCR is a site principal investigator for clinical trials supported by Eli Lilly and receives support from NIH. ALB receives research support from the NIH, the Rainwater Charitable Foundation, the Association for Frontotemporal Degeneration, Bluefield Project to Cure Frontotemporal Dementia, the Alzheimer's Drug Discovery Foundation, and the Alzheimer's Association. He has served as a consultant for Alector, AGTC, Arkuda, Arvinas, AZTherapies, GSK, Oligomerix, Ono, Regeneron, Roche, Samumed, Stealth, Third Rock, Transposon, and Wave, and received research support from Biogen, Eisai, and Regeneron. All other authors declare no competing interests.
Figures

Comment in
-
A blood test for Alzheimer's disease: a step forward.Lancet Neurol. 2021 Sep;20(9):691-693. doi: 10.1016/S1474-4422(21)00254-4. Lancet Neurol. 2021. PMID: 34418386 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
- P50 AG023501/AG/NIA NIH HHS/United States
- L30 AG069301/AG/NIA NIH HHS/United States
- K24 AG045333/AG/NIA NIH HHS/United States
- U24 AG021886/AG/NIA NIH HHS/United States
- P50 AG016574/AG/NIA NIH HHS/United States
- K24 AG053435/AG/NIA NIH HHS/United States
- R01 AG038791/AG/NIA NIH HHS/United States
- U19 AG063911/AG/NIA NIH HHS/United States
- P30 AG062422/AG/NIA NIH HHS/United States
- P01 AG019724/AG/NIA NIH HHS/United States
- U01 AG045390/AG/NIA NIH HHS/United States
- U54 NS092089/NS/NINDS NIH HHS/United States
- R01 AG045611/AG/NIA NIH HHS/United States
- K23 AG073514/AG/NIA NIH HHS/United States
- K99 AG065501/AG/NIA NIH HHS/United States
- K23 AG059888/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
