

Bridging intestinal failure with Teduglutide - A case report
- PMID: 34418803
- PMCID: PMC8384933
- DOI: 10.1016/j.ijscr.2021.106270
Bridging intestinal failure with Teduglutide - A case report
Abstract
Introduction and importance: Intestinal failure (IF) describes the state of a person's gastrointestinal absorption capabilities becoming unable to absorb fluids and nutrients needed to sustain normal physiology, leading to severe comorbidities and if left untreated, to death. IF is most commonly seen as a result of short bowel syndrome (SBS). Teduglutide is a glucagon-like peptide 2 (GLP-2) analogue used in the treatment of patients with SBS and intestinal failure (IF) as a way to reduce the need for parenteral support. Teduglutide leads to the growth of intestinal mucosa by stimulating intestinal crypt cell growth and inhibiting enterocyte apoptosis. It is usually prescribed as a final treatment step after the diagnosis of SBS-IF is made.
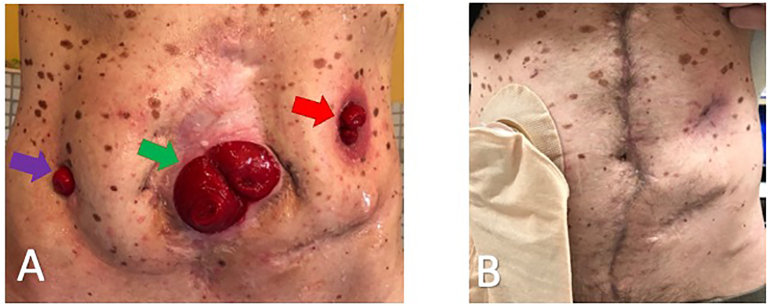
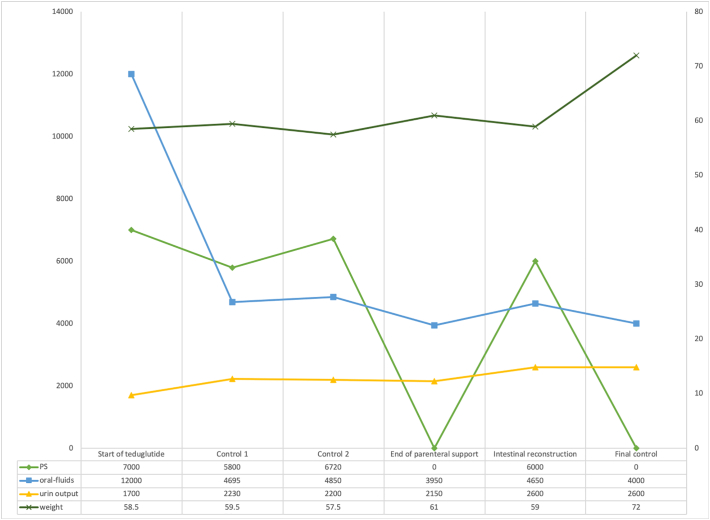
Case presentation: In this case report we present a novel strategy for using teduglutide as a bridging therapy to intestinal reconstruction. The patient achieved enteral autonomy preoperatively, underwent surgery, and remained in enteral autonomy after intestinal reconstruction.
Clinical discussion: Teduglutide has been previously exclusively used as continuous therapy in SBS-IF, this is the first reported case of using teduglutide as bridging to intestinal reconstruction. The hypothesis of this approach was to achieve an adequate nutritional status for reconstruction without the disadvantages of parenteral support.
Conclusion: The controlled application of teduglutide can provide the benefits of preoperative nutritional optimization without the disadvantages of parenteral support and at the same time facilitate an earlier and easier intestinal reconstruction.
Keywords: Bridging intestinal failure; GLP-2; Intestinal failure; Short bowel syndrome; Teduglutide.
Copyright © 2021 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
None of the authors has any conflict of interest to declare regarding this article.
Figures
References
-
- de Luis D.A., Culebras J.M., Aller R., Eiros-Bouza J.M. Surgical infection and malnutrition. Nutr. Hosp. 2014;30(3):509–513. - PubMed
-
- Mosquera C., Koutlas N.J., Edwards K.C., Strickland A., Vohra N.A., Zervos E.E. Impact of malnutrition on gastrointestinal surgical patients. J. Surg. Res. 2016;205(1):95–101. - PubMed
-
- Evans D.C., Martindale R.G., Kiraly L.N., Jones C.M. Nutrition optimization prior to surgery. Nutr. Clin. Pract. 2014;29(1):10–21. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
