

Mortality-related risk factors of COVID-19: a systematic review and meta-analysis of 42 studies and 423,117 patients
- PMID: 34418980
- PMCID: PMC8380115
- DOI: 10.1186/s12879-021-06536-3
Mortality-related risk factors of COVID-19: a systematic review and meta-analysis of 42 studies and 423,117 patients
Abstract
Background: Mortality rates of coronavirus disease-2019 (COVID-19) continue to rise across the world. The impact of several risk factors on coronavirus mortality has been previously reported in several meta-analyses limited by small sample sizes. In this systematic review, we aimed to summarize available findings on the association between comorbidities, complications, smoking status, obesity, gender, age and D-dimer, and risk of mortality from COVID-19 using a large dataset from a number of studies.
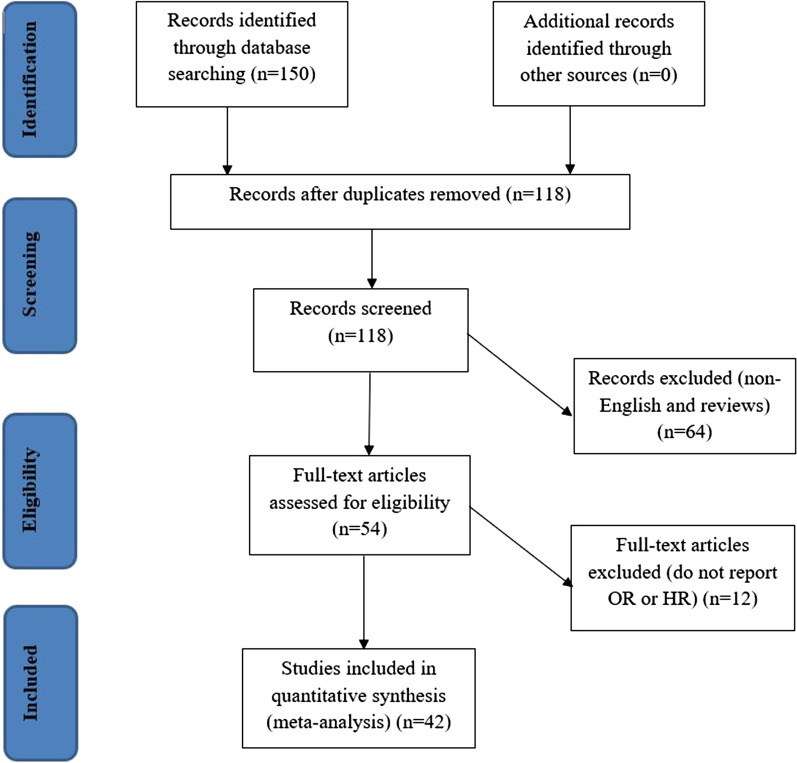
Method: Electronic databases including Google Scholar, Cochrane Library, Web of Sciences (WOS), EMBASE, Medline/PubMed, COVID-19 Research Database, and Scopus, were systematically searched till 31 August 2020. We included all human studies regardless of language, publication date or region. Forty-two studies with a total of 423,117 patients met the inclusion criteria. To pool the estimate, a mixed-effect model was used. Moreover, publication bias and sensitivity analysis were evaluated.
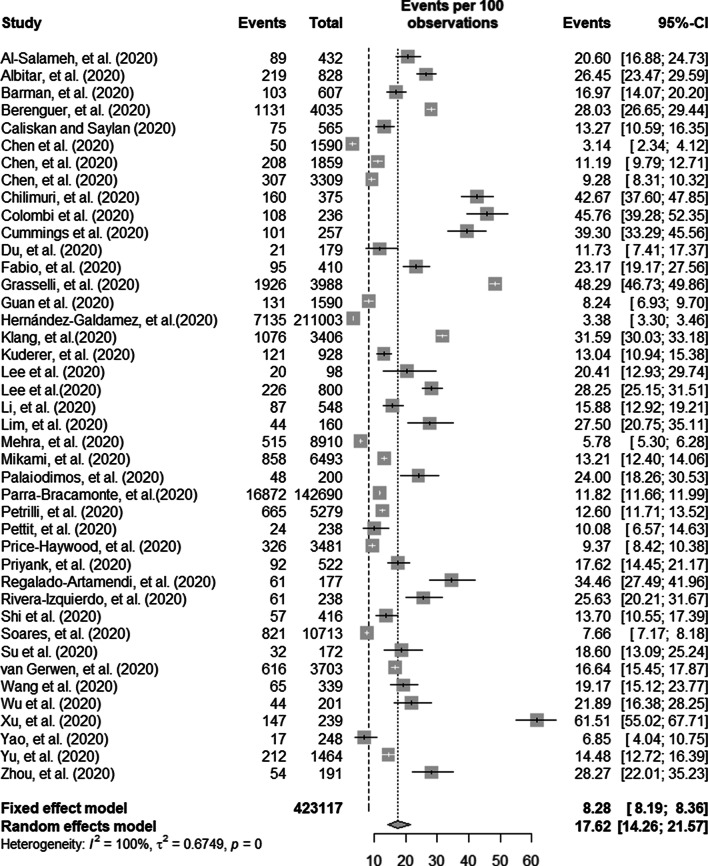
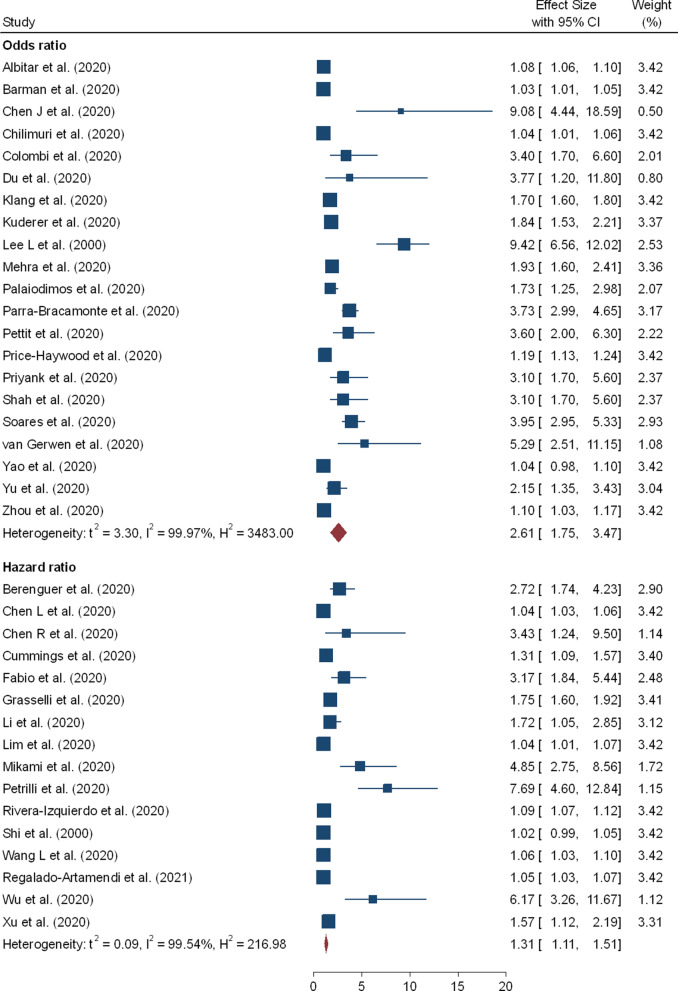
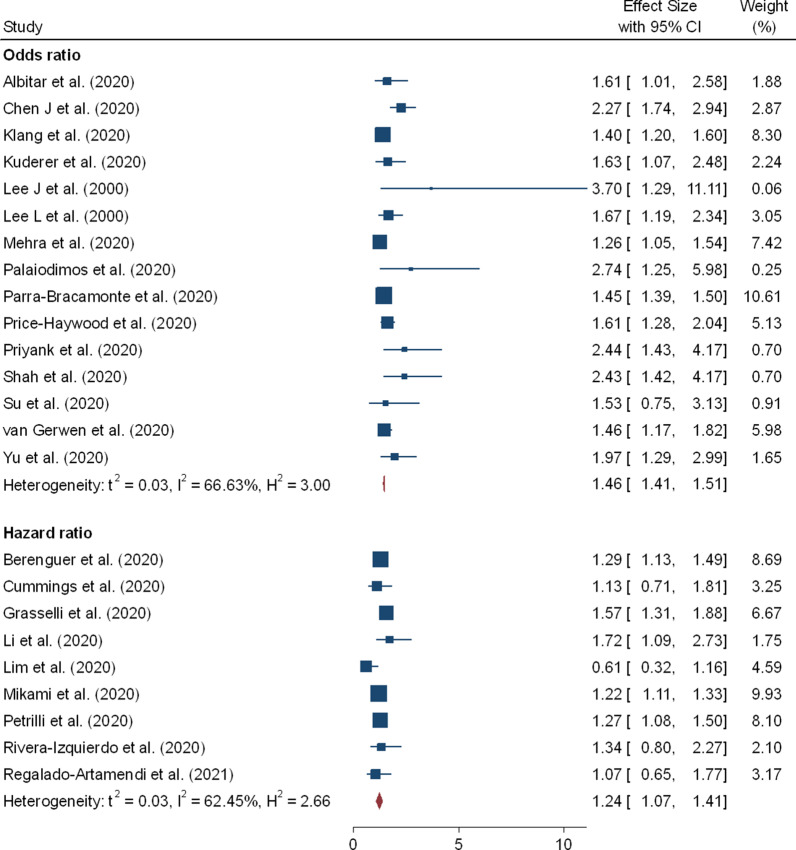
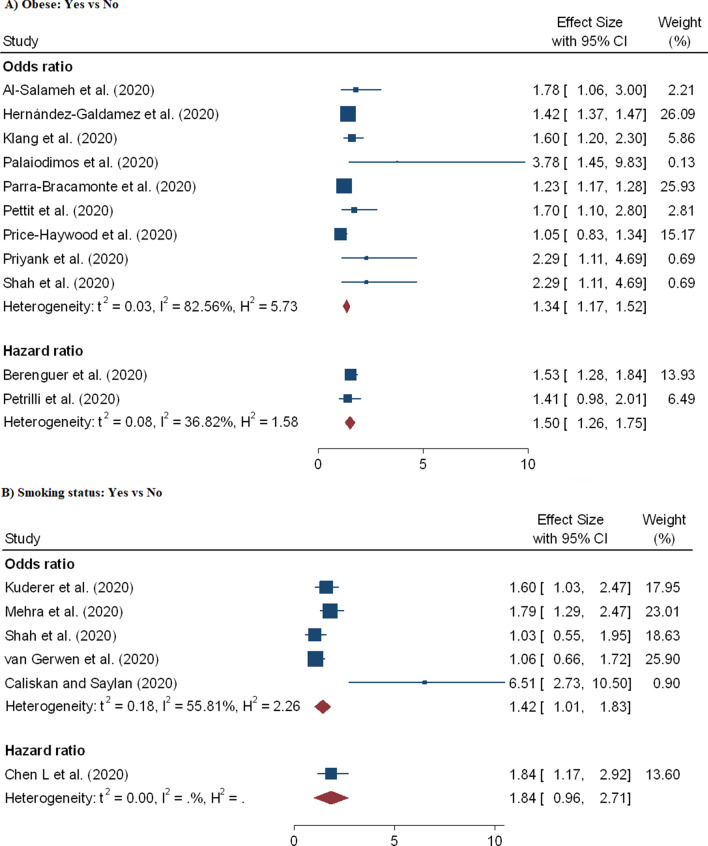
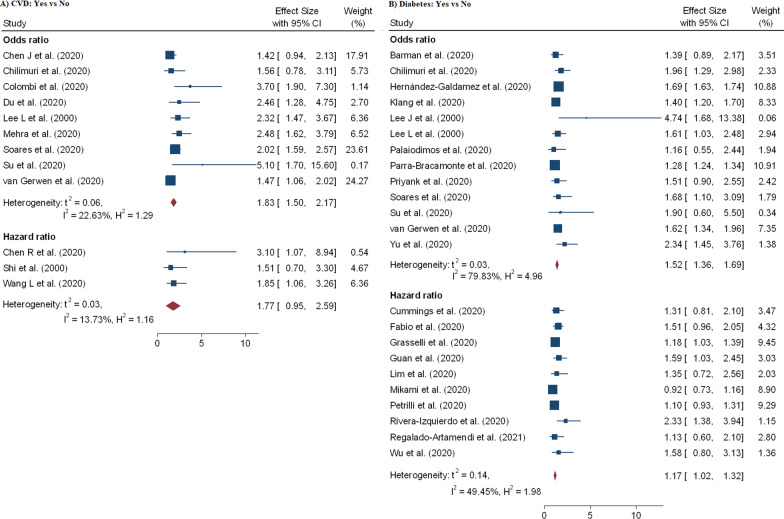
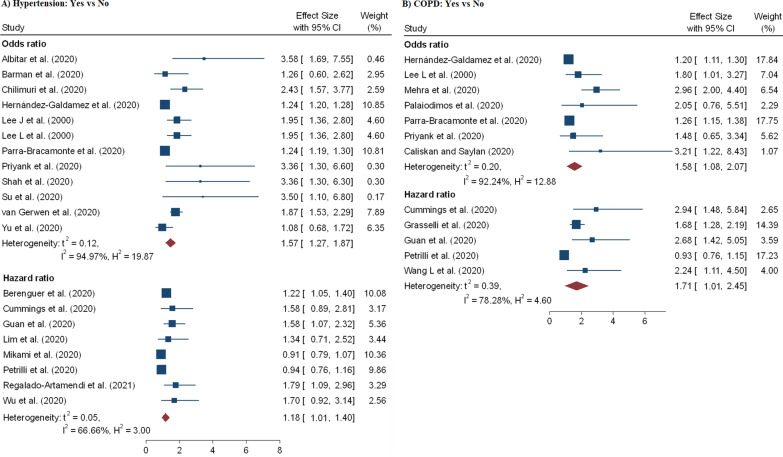
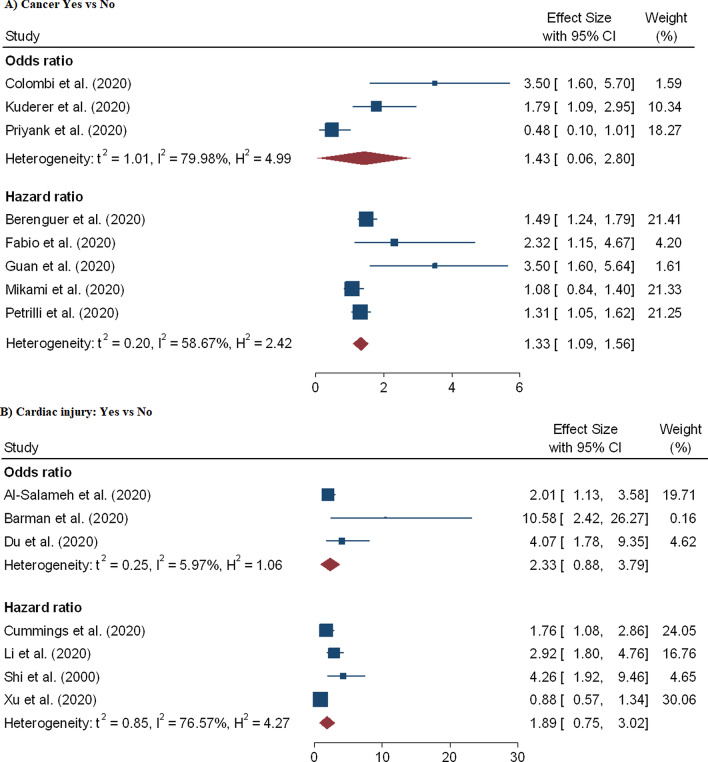
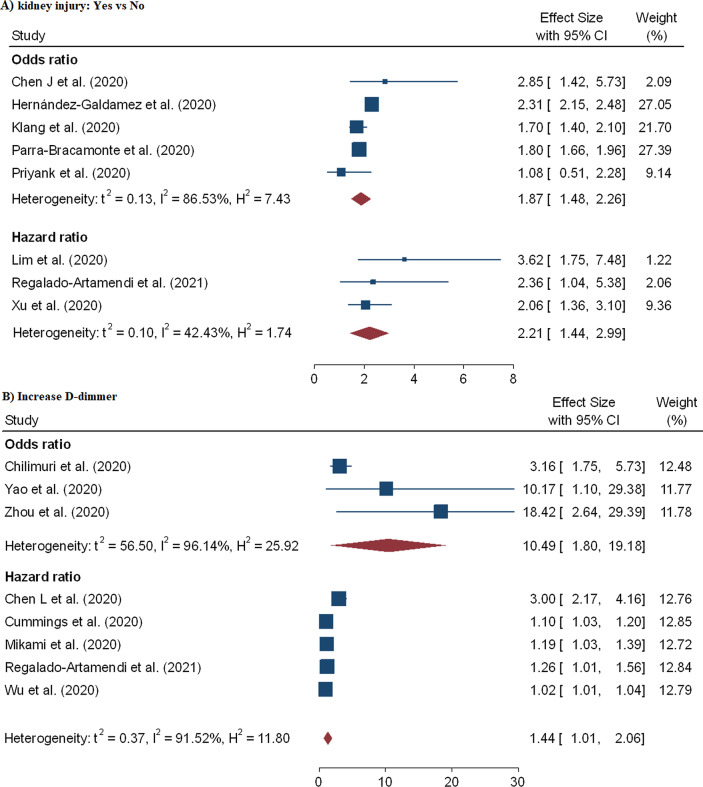
Results: The findings of the included studies were consistent in stating the contribution of comorbidities, gender, age, smoking status, obesity, acute kidney injury, and D-dimer as a risk factor to increase the requirement for advanced medical care. The analysis results showed that the pooled prevalence of mortality among hospitalized patients with COVID-19 was 17.62% (95% CI 14.26-21.57%, 42 studies and 423,117 patients). Older age has shown increased risk of mortality due to coronavirus and the pooled odds ratio (pOR) and hazard ratio (pHR) were 2.61 (95% CI 1.75-3.47) and 1.31 (95% CI 1.11-1.51), respectively. A significant association were found between COVID-19 mortality and male (pOR = 1.45; 95% CI 1.41-1.51; pHR = 1.24; 95% CI 1.07-1.41), and current smoker (pOR = 1.42; 95% CI 1.01-1.83). Furthermore, risk of mortality among hospitalized COVID-19 patients is highly influenced by patients with Chronic Obstructive Pulmonary Disease (COPD), Cardiovascular Disease (CVD), diabetes, hypertension, obese, cancer, acute kidney injury and increase D-dimer.
Conclusion: Chronic comorbidities, complications, and demographic variables including acute kidney injury, COPD, diabetes, hypertension, CVD, cancer, increased D-dimer, male gender, older age, current smoker, and obesity are clinical risk factors for a fatal outcome associated with coronavirus. The findings could be used for disease's future research, control and prevention.
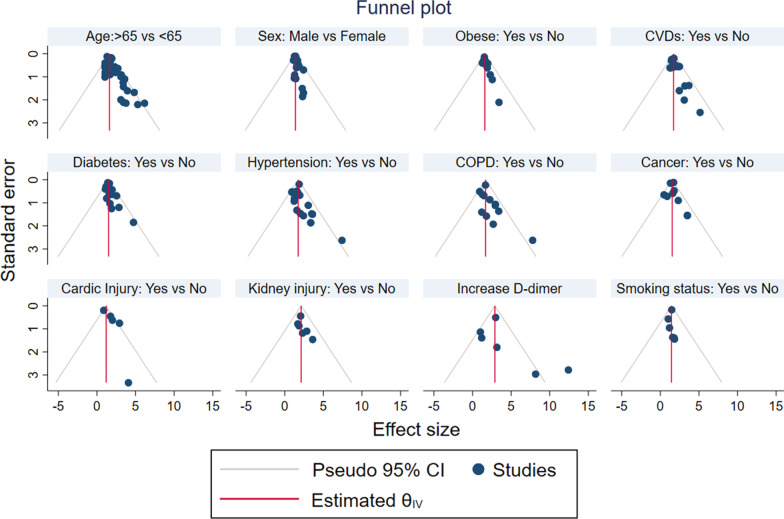
Keywords: Comorbidities; Demographic characteristics; Funnel plot; Heterogeneity; Publication bias; Sensitivity analysis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Peeri NC, Shrestha N, Rahman MS, Zaki R, Tan Z, Bibi S, Baghbanzadeh M, Aghamohammadi N, Zhang W, Haque U. The SARS, MERS and novel coronavirus (COVID-19) epidemics, the newest and biggest global health threats: what lessons have we learned? Int J Epidemiol. 2020;49:717–726. doi: 10.1093/ije/dyaa033. - DOI - PMC - PubMed
-
- Organization WH. Coronavirus disease (COVID-2019) situation reports. Geneva: World Health Organization; 2020. https://www.WHOInt/docs/default-source/coronaviruse/situationreports/202.... Accessed 15 Jan 2021.
-
- ECDC. COVID-19 situation update worldwide, as of week 2 2021updated January 2021. https://covid19-country-overviews.ecdc.europa.eu/.
-
- Abate S, Checkol Y, Mantedafro B, Basu B, Ethiopia D. Prevalence and risk factors of mortality among hospitalized patients with COVID-19: a systematic review and Meta-analysis. Bull World Health Organ. 2020 doi: 10.2471/BLT.20.260737. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
