

Norepinephrine potentiates the efficacy of volume expansion on mean systemic pressure in septic shock
- PMID: 34419120
- PMCID: PMC8379760
- DOI: 10.1186/s13054-021-03711-5
Norepinephrine potentiates the efficacy of volume expansion on mean systemic pressure in septic shock
Abstract
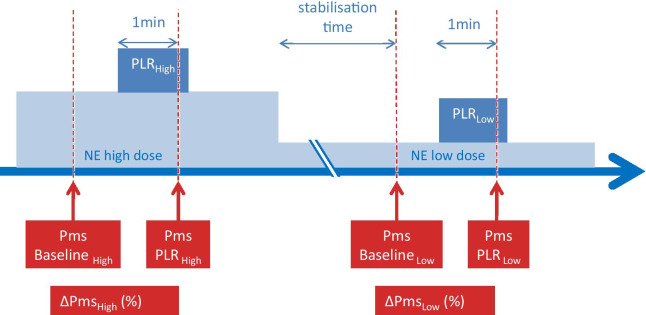
Background: Through venous contraction, norepinephrine (NE) increases stressed blood volume and mean systemic pressure (Pms) and exerts a "fluid-like" effect. When both fluid and NE are administered, Pms may not only result from the sum of the effects of both drugs. Indeed, norepinephrine may enhance the effects of volume expansion: because fluid dilutes into a more constricted, smaller, venous network, fluid may increase Pms to a larger extent at a higher than at a lower dose of NE. We tested this hypothesis, by mimicking the effects of fluid by passive leg raising (PLR).
Methods: In 30 septic shock patients, norepinephrine was decreased to reach a predefined target of mean arterial pressure (65-70 mmHg by default, 80-85 mmHg in previously hypertensive patients). We measured the PLR-induced increase in Pms (heart-lung interactions method) under high and low doses of norepinephrine. Preload responsiveness was defined by a PLR-induced increase in cardiac index ≥ 10%.
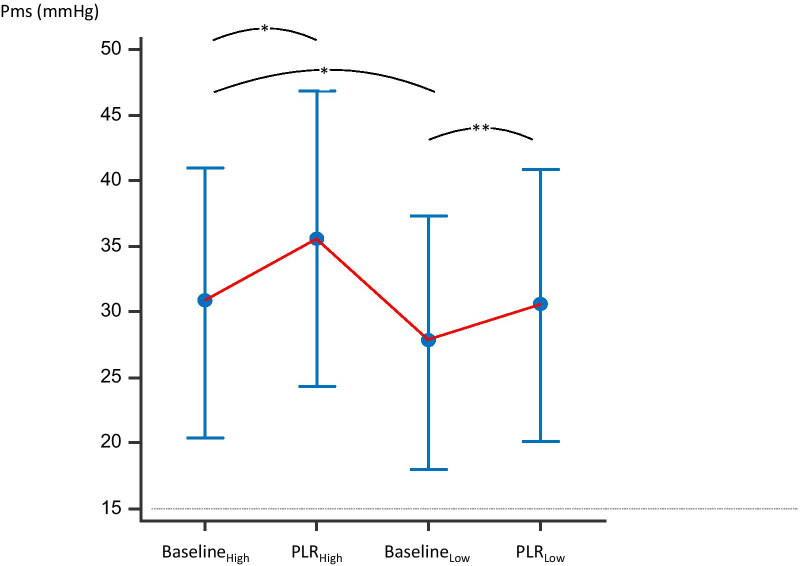
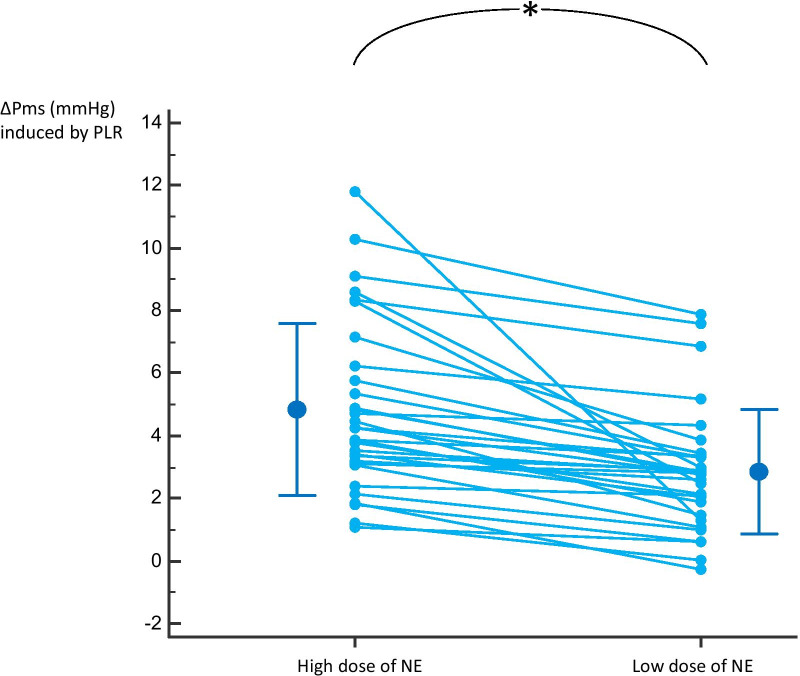
Results: Norepinephrine was decreased from 0.32 [0.18-0.62] to 0.26 [0.13-0.50] µg/kg/min (p < 0.0001). This significantly decreased the mean arterial pressure by 10 [7-20]% and Pms by 9 [4-19]%. The increase in Pms (∆Pms) induced by PLR was 13 [9-19]% at the higher dose of norepinephrine and 11 [6-16]% at the lower dose (p < 0.0001). Pms reached during PLR at the high dose of NE was higher than expected by the sum of Pms at baseline at low dose, ∆Pms induced by changing the norepinephrine dose and ∆Pms induced by PLR at low dose of NE (35.6 [11.2] mmHg vs. 33.6 [10.9] mmHg, respectively, p < 0.01). The number of preload responders was 8 (27%) at the high dose of NE and 15 (50%) at the low dose.
Conclusions: Norepinephrine enhances the Pms increase induced by PLR. These results suggest that a bolus of fluid of the same volume has a greater haemodynamic effect at a high dose than at a low dose of norepinephrine during septic shock.
Keywords: Cardiac preload; Fluid balance; Heart–lung interactions; Vasopressors; Venous return.
© 2021. The Author(s).
Conflict of interest statement
J-LT and XM are members of the medical advisory board of Pulsion Medical Systems, Getinge. The other authors have no conflict of interest to declare.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
