

Incidence of acute rheumatic fever in northern and western Uganda: a prospective, population-based study
- PMID: 34419237
- PMCID: PMC11144057
- DOI: 10.1016/S2214-109X(21)00288-6
Incidence of acute rheumatic fever in northern and western Uganda: a prospective, population-based study
Abstract
Background: Acute rheumatic fever is infrequently diagnosed in sub-Saharan African countries despite the high prevalence of rheumatic heart disease. We aimed to determine the incidence of acute rheumatic fever in northern and western Uganda.
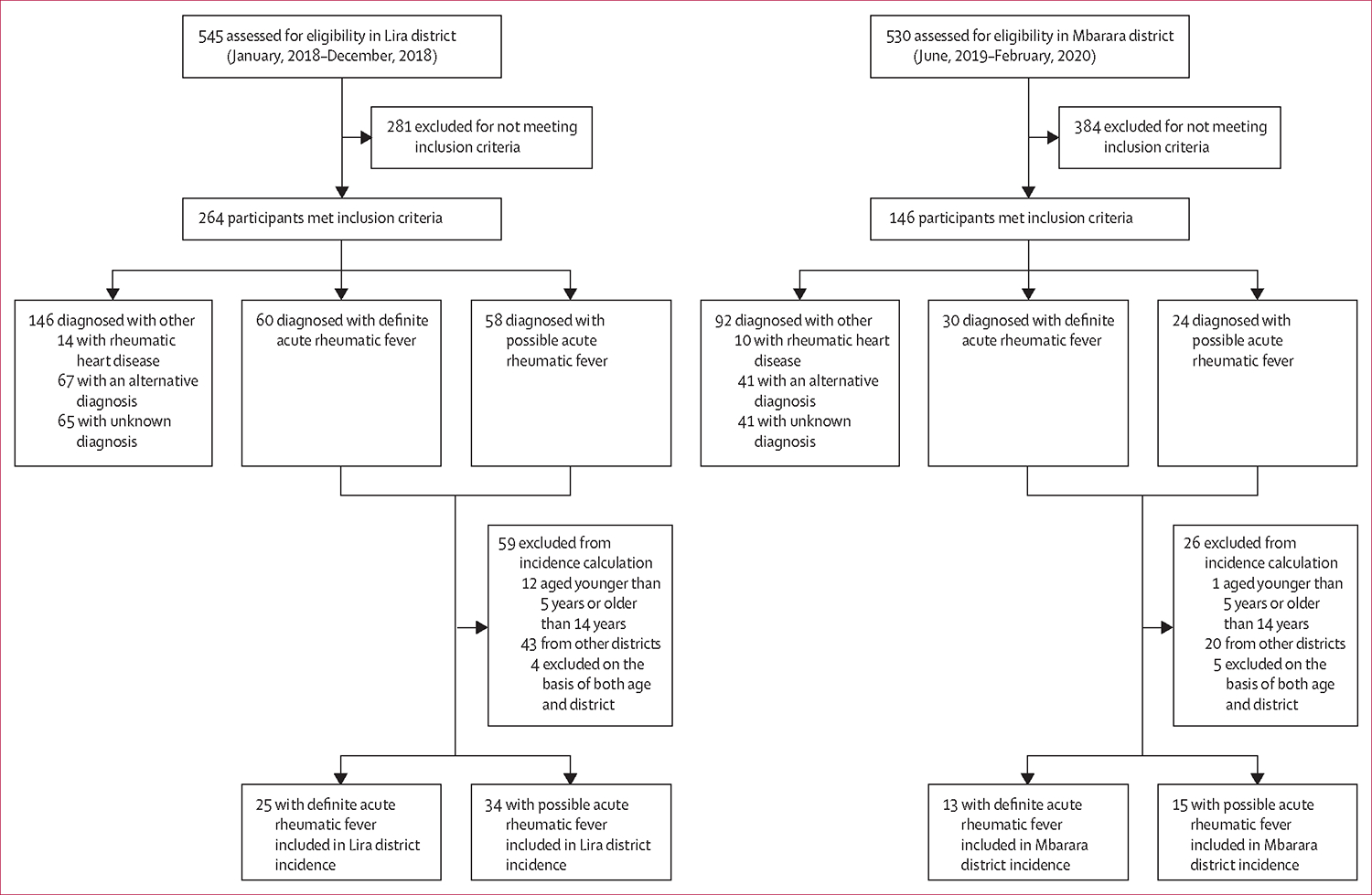
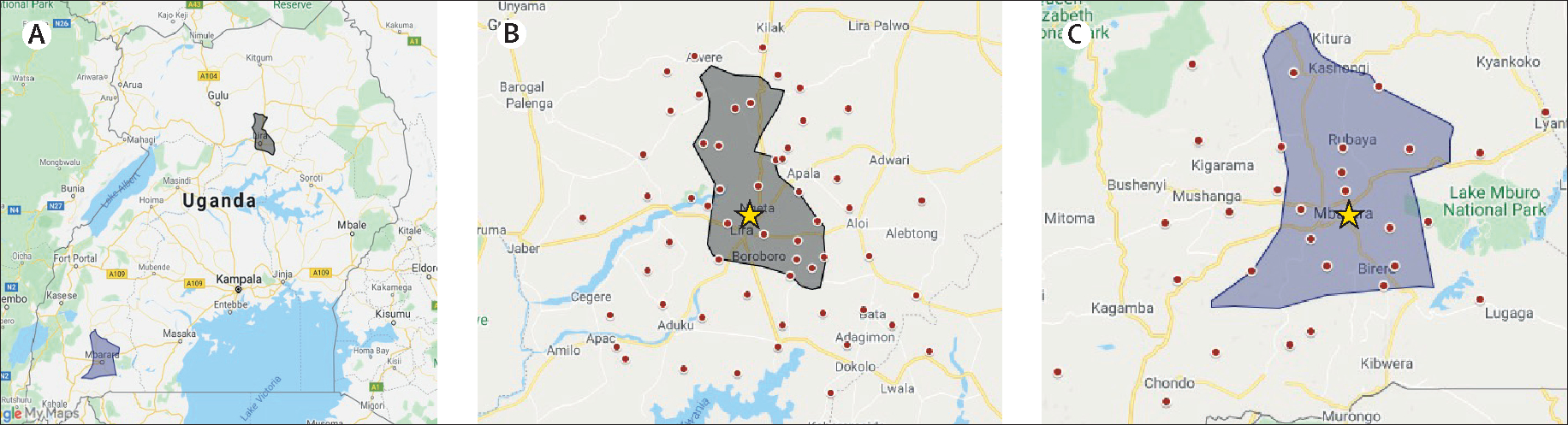
Methods: For our prospective epidemiological study, we established acute rheumatic fever clinics at two regional hospitals in the north (Lira district) and west (Mbarara district) of Uganda and instituted a comprehensive acute rheumatic fever health messaging campaign. Communities and health-care workers were encouraged to refer children aged 3-17 years, with suspected acute rheumatic fever, for a definitive diagnosis using the Jones Criteria. Children were referred if they presented with any of the following: (1) history of fever within the past 48 h in combination with any joint complaint, (2) suspicion of acute rheumatic carditis, or (3) suspicion of chorea. We excluded children with a confirmed alternative diagnosis. We estimated incidence rates among children aged 5-14 years and characterised clinical features of definite and possible acute rheumatic fever cases.
Findings: Data were collected between Jan 17, 2018, and Dec 30, 2018, in Lira district and between June 5, 2019, and Feb 28, 2020, in Mbarara district. Of 1075 children referred for evaluation, 410 (38%) met the inclusion criteria; of these, 90 (22%) had definite acute rheumatic fever, 82 (20·0%) had possible acute rheumatic fever, and 24 (6%) had rheumatic heart disease without evidence of acute rheumatic fever. Additionally, 108 (26%) children had confirmed alternative diagnoses and 106 (26%) had an unknown alternative diagnosis. We estimated the incidence of definite acute rheumatic fever among children aged 5-14 years as 25 cases (95% CI 13·7-30·3) per 100 000 person-years in Lira district (north) and 13 cases (7·1-21·0) per 100 000 person-years in Mbarara district (west).
Interpretation: To the best of our knowledge, this is the first population-based study to estimate the incidence of acute rheumatic fever in sub-Saharan Africa. Given the known rheumatic heart disease burden, it is likely that only a proportion of children with acute rheumatic fever were diagnosed. These data dispel the long-held hypothesis that the condition does not exist in sub-Saharan Africa and compel investment in improving prevention, recognition, and diagnosis of acute rheumatic fever.
Funding: American Heart Association Children's Strategically Focused Research Network Grant, THRiVE-2, General Electric, and Cincinnati Children's Heart Institute Research Core.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests TP reports grant funding from the National Institute for Health Research (ACF-2016-20-001). All other authors declare no competing interests.
Figures
Comment on
-
Long-awaited update on estimates of acute rheumatic fever in Africa.Lancet Glob Health. 2021 Oct;9(10):e1347-e1348. doi: 10.1016/S2214-109X(21)00344-2. Epub 2021 Aug 19. Lancet Glob Health. 2021. PMID: 34419238 No abstract available.
References
-
- WHO. Rheumatic fever and rheumatic heart disease. Geneva: Switzerland, 2018.
-
- Beaton A, Okello E, Lwabi P, Mondo C, McCarter R, Sable C. Echocardiography screening for rheumatic heart disease in Ugandan schoolchildren. Circulation 2012; 125: 3127–32. - PubMed
-
- Sims Sanyahumbi A, Sable CA, Beaton A, et al. School and community screening shows Malawi, Africa, to have a high prevalence of latent rheumatic heart disease. Congenit Heart Dis 2016; 11: 615–21. - PubMed
-
- Tibazarwa KB, Volmink JA, Mayosi BM. Incidence of acute rheumatic fever in the world: a systematic review of population-based studies. Heart 2008; 94: 1534–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
