

Role of Exercise Treadmill Testing in the Assessment of Coronary Microvascular Disease
- PMID: 34419395
- PMCID: PMC8831663
- DOI: 10.1016/j.jcmg.2021.07.013
Role of Exercise Treadmill Testing in the Assessment of Coronary Microvascular Disease
Abstract
Objectives: The authors aimed to study the sensitivity and specificity of exercise treadmill testing (ETT) in the diagnosis of coronary microvascular disease (CMD), as well as the prognostic implications of ETT results in patients with CMD.
Background: ETT is validated to evaluate for flow-limiting coronary artery disease (CAD), however, little is known about its use for evaluating CMD.
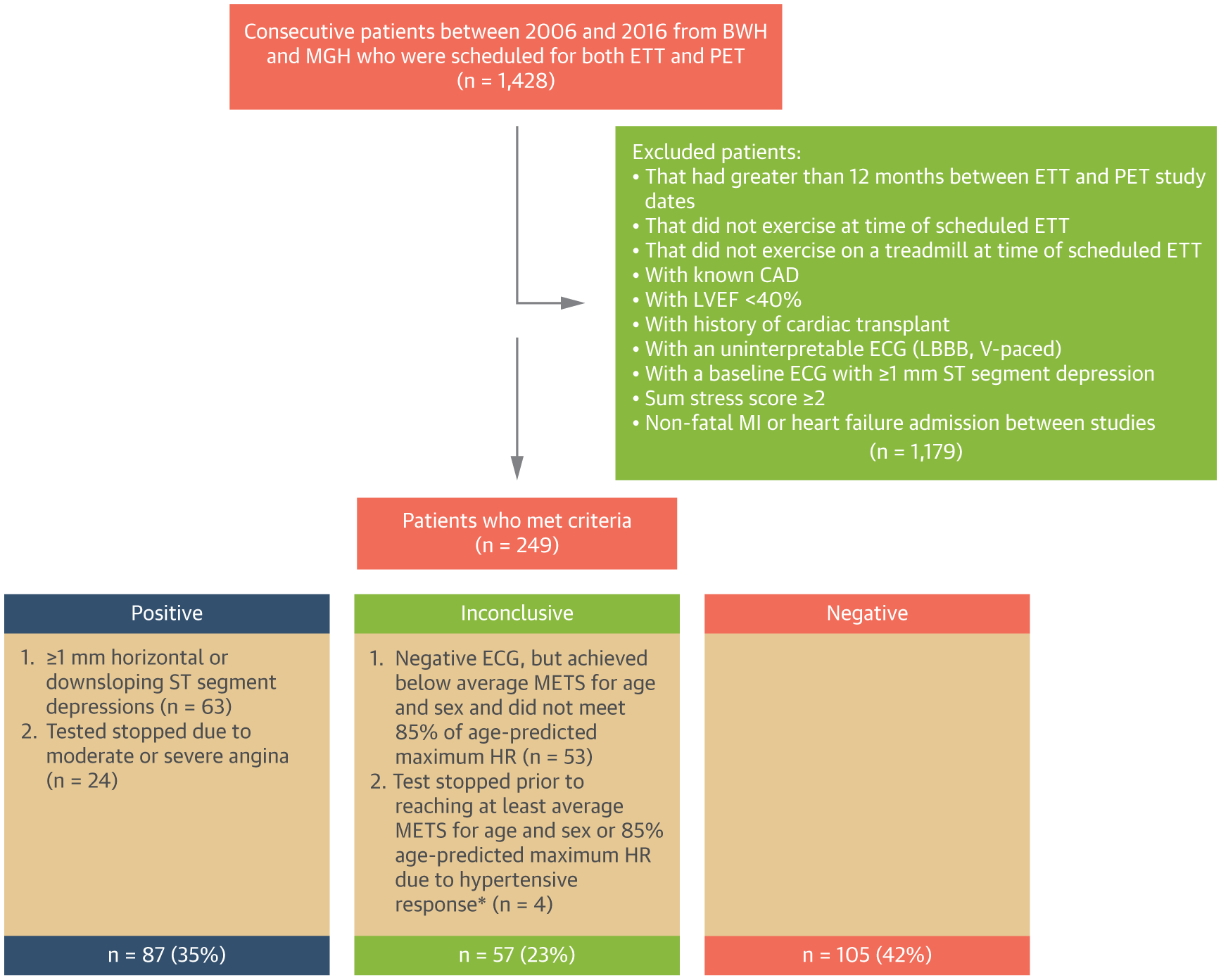
Methods: We retrospectively studied 249 consecutive patients between 2006 and 2016 who underwent ETT and positron emission tomography within 12 months. Patients with obstructive CAD or left ventricular systolic dysfunction were excluded. CMD was defined as a coronary flow reserve <2. Patients were followed for the occurrence of a first major adverse event (composite of death or hospitalization for myocardial infarction or heart failure).
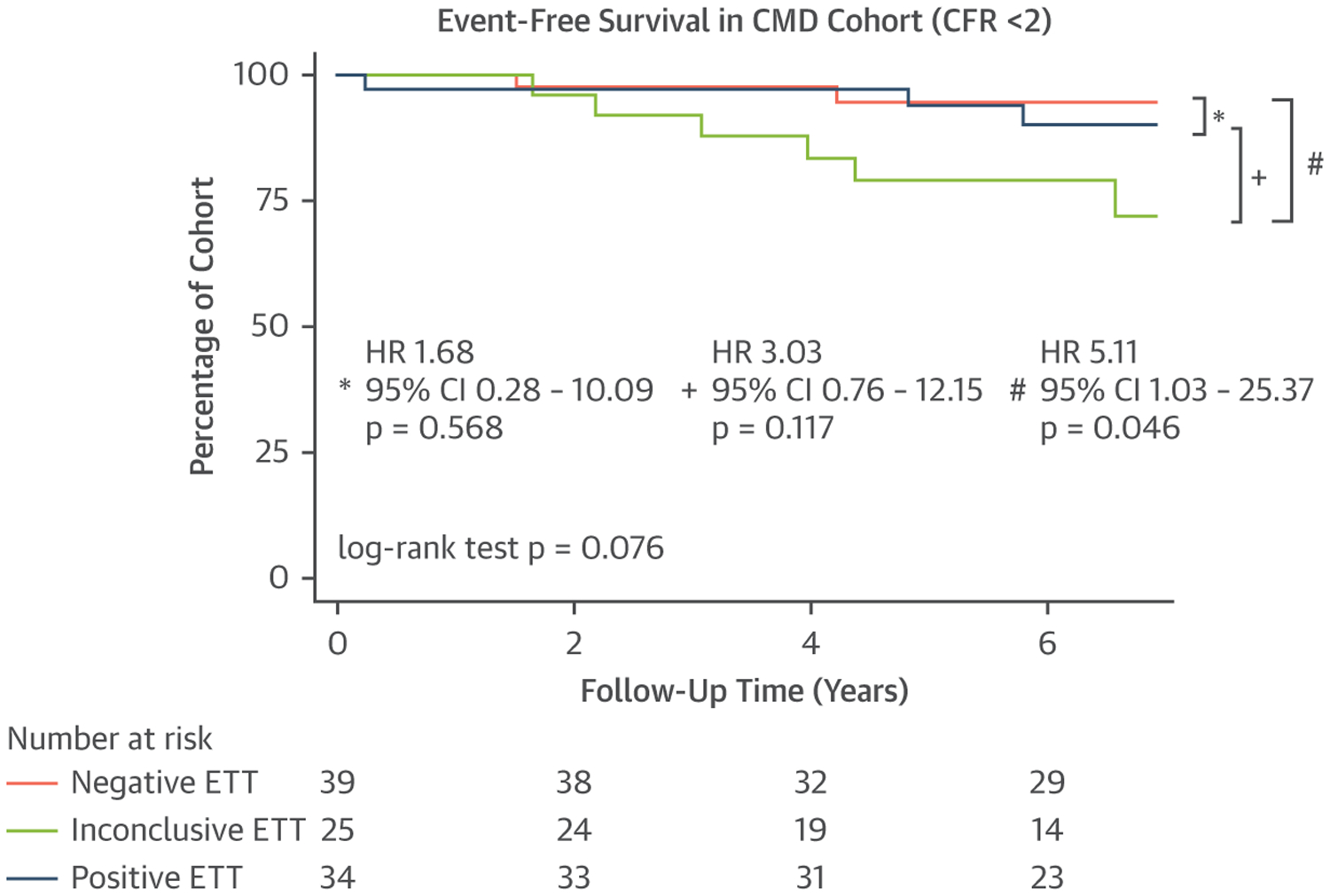
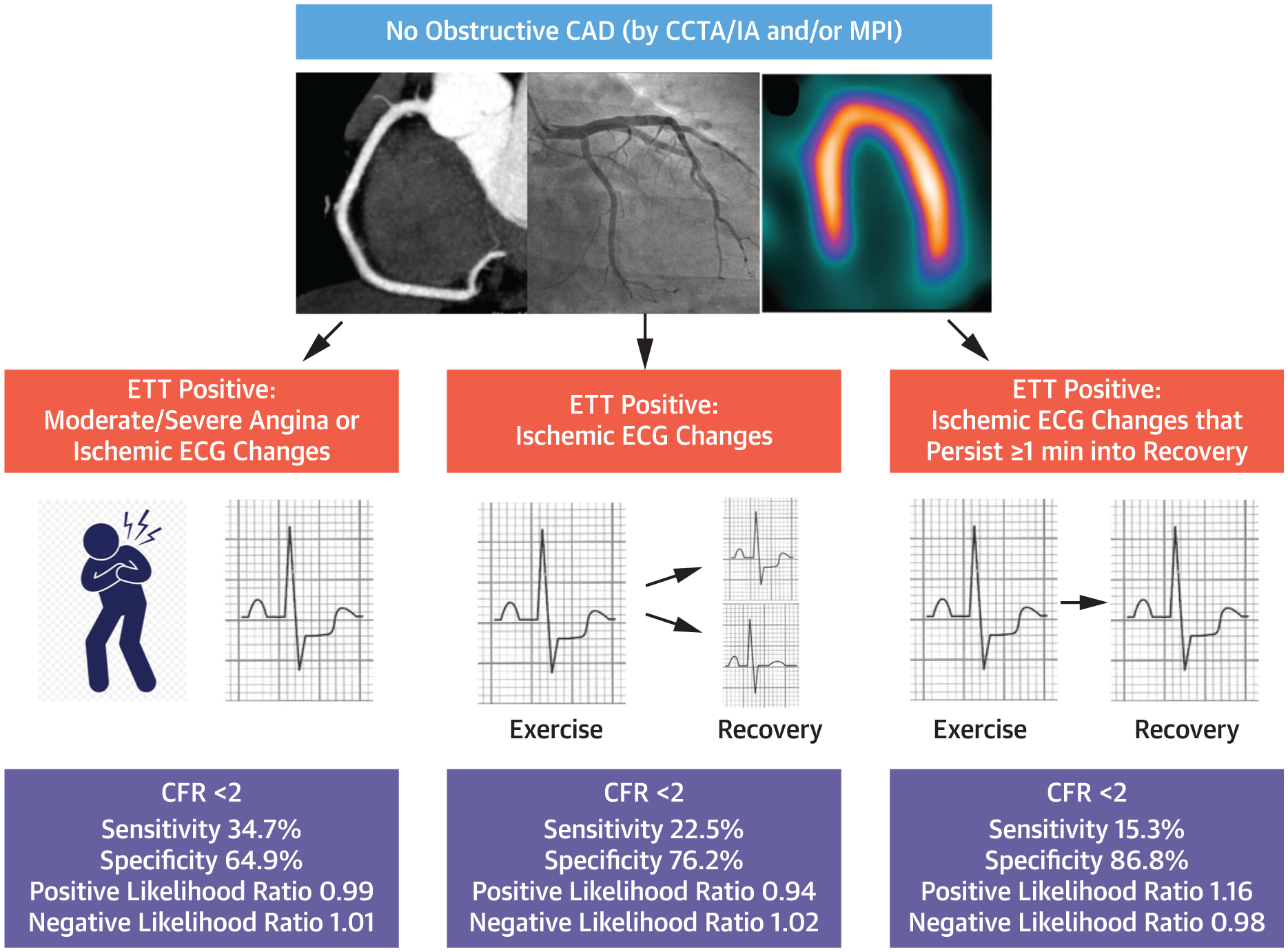
Results: The sensitivity and specificity of a positive ETT to detect CMD were 34.7% (95% CI: 25.4%-45.0%) and 64.9% (95% CI: 56.7%-72.5%), respectively. The specificity of a positive ETT to detect CMD increased to 86.8% (95% CI: 80.3%-91.7%) when only classifying studies with ischemic electrocardiogram changes that lasted at least 1 minute into recovery as positive, although at a cost of lower sensitivity (15.3%; 95% CI: 8.8%-24.0%). Over a median follow-up of 6.9 years (IQR: 5.1-8.2 years), 30 (12.1%) patients met the composite endpoint, including 13 (13.3%) with CMD (n = 98). In patients with CMD, ETT result was not associated with the composite endpoint (P = 0.076).
Conclusions: Our data suggest limited sensitivity of ETT to detect CMD. However, a positive ETT with ischemic changes that persist at least 1 minute into recovery in the absence of obstructive CAD should raise suspicion for the presence of CMD given a high specificity. Further study is needed with larger patient sample sizes to assess the association between ETT results and outcomes in patients with CMD.
Keywords: coronary flow reserve; coronary microvascular disease; exercise stress testing.
Copyright © 2022. Published by Elsevier Inc.
Conflict of interest statement
Funding Support and Author Disclosures Dr Divakaran has received a T32 postdoctoral training grant from the National Heart, Lung, and Blood Institute (T32 HL094301) and a joint KL2/Catalyst Medical Research Investigator Training (CMeRIT) award from Harvard Catalyst and the Boston Claude D. Pepper Older Americans Independence Center (5P30AG031679-10). Dr Zhou has received a T32 postdoctoral training grant from the National Heart, Lung, and Blood Institute (T32 HL094301). Dr Osborne has received a KL2/Catalyst Medical Research Investigator Training award (an appointed KL2 award) from Harvard Catalyst/The Harvard Clinical and Translational Science Center (National Center for Advancing Translational Sciences, National Institutes of Health Award KL2 TR002542). Dr Taqueti has received grant number K23 HL135438 from the National Heart, Lung, and Blood Institute. Dr Dorbala has received grant number R01 HL130563 from the National Heart, Lung, and Blood Institute. Dr Di Carli has received grant number R01 HL132021 from the National Heart, Lung, and Blood Institute. This work was conducted with support from Harvard Catalyst/The Harvard Clinical and Translational Science Center (National Center for Advancing Translational Sciences, National Institutes of Health Award UL 1TR002541) and financial contributions from Harvard University and its affiliated academic health care centers. The content is solely the responsibility of the authors and does not necessarily represent the official views of Harvard Catalyst, Harvard University, and its affiliated academic health care centers, or the National Institutes of Health. Dr Osborne has served as a consultant for Intrinsic Imaging, LLC. Dr Dorbala is a member of an advisory board for General Electric Health Care. Dr Di Carli has received research grant support from Spectrum Dynamics and consulting fees from Sanofi and General Electric. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Rethinking the Goal of Exercise Tolerance Testing: Identifying Ischemic Heart Disease, Whether Epicardial or Microvascular.JACC Cardiovasc Imaging. 2022 Feb;15(2):322-324. doi: 10.1016/j.jcmg.2021.10.010. Epub 2021 Dec 15. JACC Cardiovasc Imaging. 2022. PMID: 34922862 No abstract available.
References
-
- Jespersen L, Hvelplund A, Abildstrøm SZ, et al. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur Heart J. 2012;33:734–744. - PubMed
-
- Ford TJ, Stanley B, Good R, et al. Stratified medical therapy using invasive coronary function testing in angina: The CorMicA Trial. J Am Coll Cardiol. 2018;72:2841–2855. - PubMed
-
- Ong P, Camici PG, Beltrame JF, et al. International standardization of diagnostic criteria for microvascular angina. Int J Cardiol. 2018;250:16–20. - PubMed
-
- Ford TJ, Ong P, Sechtem U, et al. Assessment of vascular dysfunction in patients without obstructive coronary artery disease: why, how, and when. J Am Coll Cardiol Intv. 2020;13:1847–1864. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
