

Handheld ultrasound in training - The future is getting smaller!
- PMID: 34422105
- PMCID: PMC8373282
- DOI: 10.1177/1751143720914216
Handheld ultrasound in training - The future is getting smaller!
Abstract
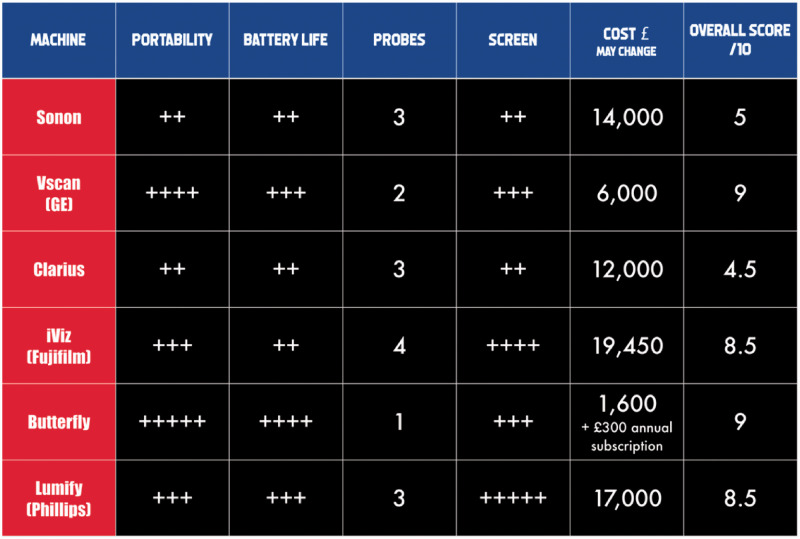
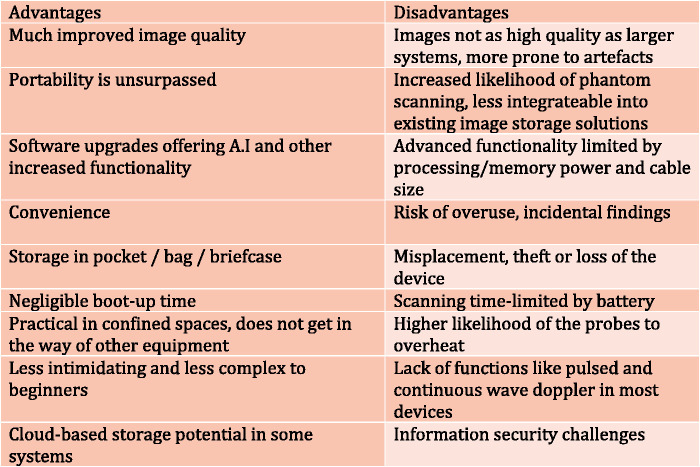
Traditional ultrasound teaching is normally delivered using large, costly and often quite advanced cart-based systems. These carts are often large systems on wheels, usually limited to the departments that own them i.e. clinics, wards or radiology. Portability has been further improved by the development of laptop style systems, which are easier to wheel in-between patients/departments. In our experience and anecdotally, many of these systems can be intimidating to the novice and can lead to early attrition or poor uptake of ultrasound into clinical practice. Carts can also restrict the amount of training deliverable to practitioners, as they are limited in number due to cost and can take quite some time to boot up, reducing convenience. This dogma is being progressively changed with the advent of smaller handheld devices, some clearly within the financial grasps of most practitioners, and even to the point of medical schools offering students their own personal device.1,2 This relative inexpensiveness can lead to the purchase of these devices for novelty and convenience, over need. Obvious caution is needed in these circumstances, but with increased ease of purchase, better availability and inbuilt simplicity, ultrasound learning can be seamlessly integrated into day-to-day practice. This review discusses how one of the most disruptive innovations in modern medicine is changing ultrasound from a classic imaging modality to become integrated as the fifth pillar of clinical examination, and how these new devices can serve as springboards to more advanced ultrasound training. In fact, within what has become a bigger area of clinical examination, things are getting smaller.
Keywords: Ultrasound; handheld ultrasound; pocket ultrasound; point of care; point of care ultrasound; training.
© The Intensive Care Society 2020.
Figures
References
-
- https://www.itnonline.com/content/mount-sinai-school-medicine-gives-pock... (accessed 2 November 2019).
-
- https://www.mobihealthnews.com/news/north-america/uc-irvine-medical-scho... (accessed 3 November 2019).
-
- Elder A, Japp A, Verghese A. How valuable is physical examination of the cardiovascular system? Br Med J 2016; 354: i3309. - PubMed
-
- Mehta M, Jacobson T, Peters D, et al.Handheld ultrasound versus physical examination in patients referred for transthoracic echocardiography for a suspected cardiac condition. JACC Cardiovasc Imaging 2014; 7: 983–990. - PubMed
LinkOut - more resources
Full Text Sources