

A simple assessment of lung nodule location for reduction in unnecessary invasive procedures
- PMID: 34422349
- PMCID: PMC8339782
- DOI: 10.21037/jtd-20-3093
A simple assessment of lung nodule location for reduction in unnecessary invasive procedures
Abstract
Background: CT screening for lung cancer results in a significant mortality reduction but is complicated by invasive procedures performed for evaluation of the many detected benign nodules. The purpose of this study was to evaluate measures of nodule location within the lung as predictors of malignancy.
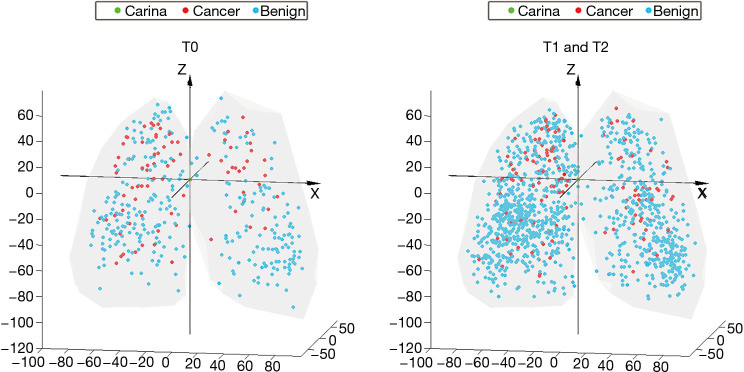
Methods: We analyzed images and data from 3,483 participants in the National Lung Screening Trial (NLST). All nodules (4-20 mm) were characterized by 3D geospatial location using a Cartesian coordinate system and evaluated in logistic regression analysis. Model development and probability cutpoint selection was performed in the NLST testing set. The Geospatial test was then validated in the NLST testing set, and subsequently replicated in a new cohort of 147 participants from The Detection of Early Lung Cancer Among Military Personnel (DECAMP) Consortium.
Results: The Geospatial Test, consisting of the superior-inferior distance (Z distance), nodule diameter, and radial distance (carina to nodule) performed well in both the NLST validation set (AUC 0.85) and the DECAMP replication cohort (AUC 0.75). A negative Geospatial Test resulted in a less than 2% risk of cancer across all nodule diameters. The Geospatial Test correctly reclassified 19.7% of indeterminate nodules with a diameter over 6mm as benign, while only incorrectly classifying 1% of cancerous nodules as benign. In contrast, the parsimonious Brock Model applied to the same group of nodules correctly reclassified 64.5% of indeterminate nodules as benign but resulted in misclassification of a cancer as benign in 18.2% of the cases. Applying the Geospatial test would result in reducing invasive procedures performed for benign lesions by 11.3% with a low rate of misclassification (1.3%). In contrast, the Brock model applied to the same group of patients results in decreasing invasive procedures for benign lesion by 39.0% but misclassifying 21.1% of cancers as benign.
Conclusions: Utilizing information about geospatial location within the lung improves risk assessment for indeterminate lung nodules and may reduce unnecessary procedures.
Trial registration: NCT00047385, NCT01785342.
Keywords: Lung nodule; nodule location; non-small cell lung cancer.
2021 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://dx.doi.org/10.21037/jtd-20-3093). CMK reports grant funding from the NIH, consulting fees and clinical trial funding from Johnson and Johnson. CMK is a consultant and equity holder for Quantitative Imaging Solutions, and sits on the Board of Directors of the American Association of Bronchology and Interventional Pulmonology and the Prevention Committee of the Alliance for Oncology Clinical Trials. EB reports grant funding from the Department of Defense, Johnson and Johnson, and the National Cancer Institute. VM reports funding from the Damon Runyon Cancer Research Foundation and CAPES (Brazil). HM reports grant funding from Novartis, Janssen, and the Department of Defense. BT, AC, and ID, and Ruben SJ report consulting fees from Quantitative Imaging Services. CS reports Johnson and Johnson funding for DECAMP, and is employed by and owns stock in Johnson and Johnson. DA reports grant funding from American College of Radiology, Boston University, the NIH, and the Kaiser Foundation/PCORI, honoraria from the NIH, Department of Defense, International Symposium on Clinical Update in Respiratory Medicine, Cancer Research UC, American Lung Association, Japanese Society for CT screening, and grant support from the Early Detection Research Network, Molecular and Cellular Characterization of Screen-Detected Lesions Consortium, Department of Defense, International Lung Cancer Conference, Early Detection of Cancer Conference, and the Molecular and Cellular Characterization of Screen-Detected Lesions Consortium, support for meetings/travel from the American Institute for Medical and Biological Engineering, Cleveland Clinic, Specialized Programs of Research Excellence, and the International Association for the Study of Lung Cancer. JHB reports consulting fees from Johnson and Johnson. AS is an employee of Johnson and Johnson. GRW is an equity holder in Quantitative Imaging Solutions. RSJ reports grants from the NIH, a patent pending in lung cancer risk assessment, and is an equity holder of Quantitative Imaging Solutions. The authors have no other conflicts of interest to declare.
Figures

References
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical