

Age-Adjusted Associations Between Comorbidity and Outcomes of COVID-19: A Review of the Evidence From the Early Stages of the Pandemic
- PMID: 34422736
- PMCID: PMC8377370
- DOI: 10.3389/fpubh.2021.584182
Age-Adjusted Associations Between Comorbidity and Outcomes of COVID-19: A Review of the Evidence From the Early Stages of the Pandemic
Abstract
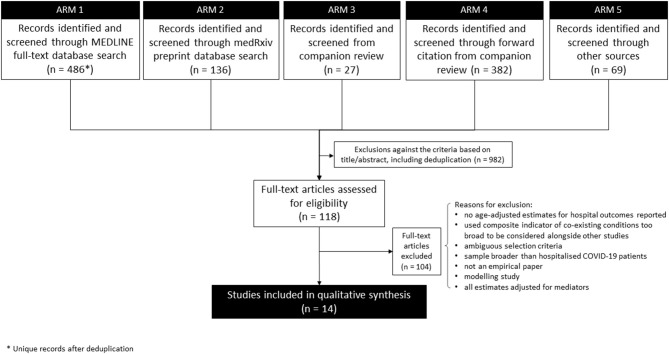
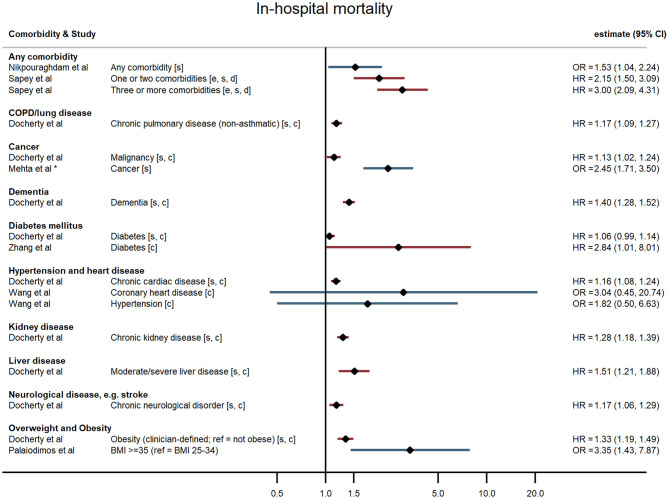
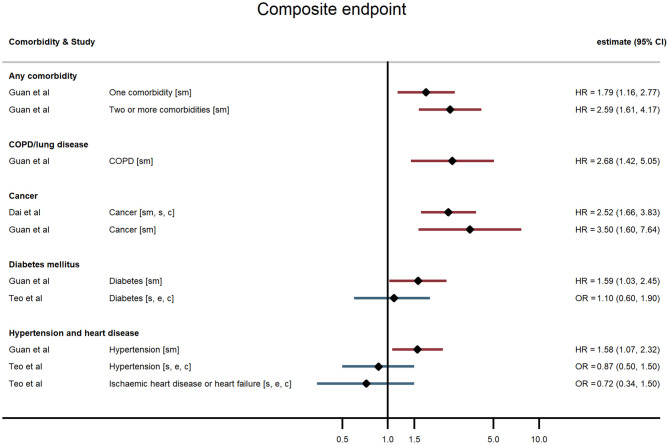
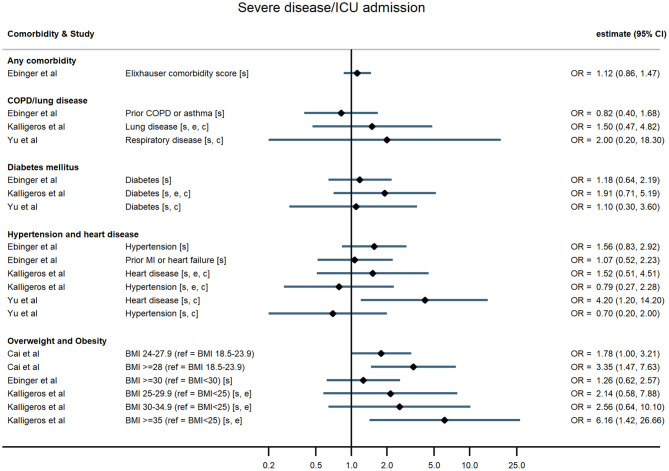
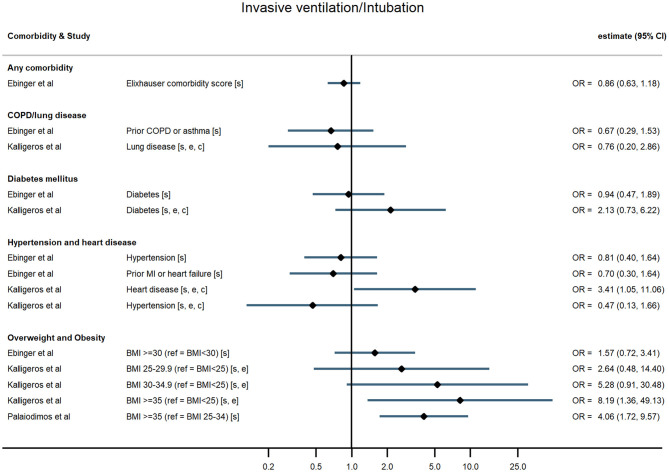
Objectives: Early in the COVID-19 pandemic, people with underlying comorbidities were overrepresented in hospitalised cases of COVID-19, but the relationship between comorbidity and COVID-19 outcomes was complicated by potential confounding by age. This review therefore sought to characterise the international evidence base available in the early stages of the pandemic on the association between comorbidities and progression to severe disease, critical care, or death, after accounting for age, among hospitalised patients with COVID-19. Methods: We conducted a rapid, comprehensive review of the literature (to 14 May 2020), to assess the international evidence on the age-adjusted association between comorbidities and severe COVID-19 progression or death, among hospitalised COVID-19 patients - the only population for whom studies were available at that time. Results: After screening 1,100 studies, we identified 14 eligible for inclusion. Overall, evidence for obesity and cancer increasing risk of severe disease or death was most consistent. Most studies found that having at least one of obesity, diabetes mellitus, hypertension, heart disease, cancer, or chronic lung disease was significantly associated with worse outcomes following hospitalisation. Associations were more consistent for mortality than other outcomes. Increasing numbers of comorbidities and obesity both showed a dose-response relationship. Quality and reporting were suboptimal in these rapidly conducted studies, and there was a clear need for additional studies using population-based samples. Conclusions: This review summarises the most robust evidence on this topic that was available in the first few months of the pandemic. It was clear at this early stage that COVID-19 would go on to exacerbate existing health inequalities unless actions were taken to reduce pre-existing vulnerabilities and target control measures to protect groups with chronic health conditions.
Keywords: COVID-19; chronic disease; comorbidity; coronavirus; review.
Copyright © 2021 Mason, Maudsley, McHale, Pennington, Day and Barr.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Center for Systems Science and Engineering . COVID-19 Dashboard Johns Hopkins University. (2020). Available online at: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594... (accessed June 22, 2021).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical