

Clinical characteristics of the first and second COVID-19 waves in the Bronx, New York: A retrospective cohort study
- PMID: 34423331
- PMCID: PMC8367084
- DOI: 10.1016/j.lana.2021.100041
Clinical characteristics of the first and second COVID-19 waves in the Bronx, New York: A retrospective cohort study
Abstract
Background: There is limited clinical patient data comparing the first and second waves of the coronavirus disease 2019 (COVID-19) in the United States and the effects of a COVID-19 resurgence on different age, racial and ethnic groups. We compared the first and second COVID-19 waves in the Bronx, New York, among a racially and ethnically diverse population.
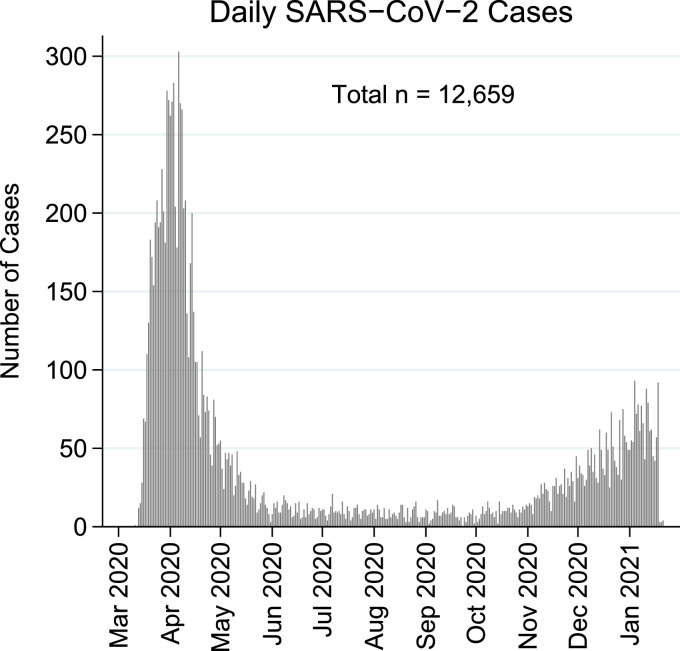
Methods: Patients in this retrospective cohort study were included if they had a laboratory-confirmed SARS-CoV-2 infection by a real-time PCR test of a nasopharyngeal swab specimen detected between March 11, 2020, and January 21, 2021. Main outcome measures were critical care, in-hospital acquired disease and death. Patient demographics, comorbidities, vitals, and laboratory values were also collected.
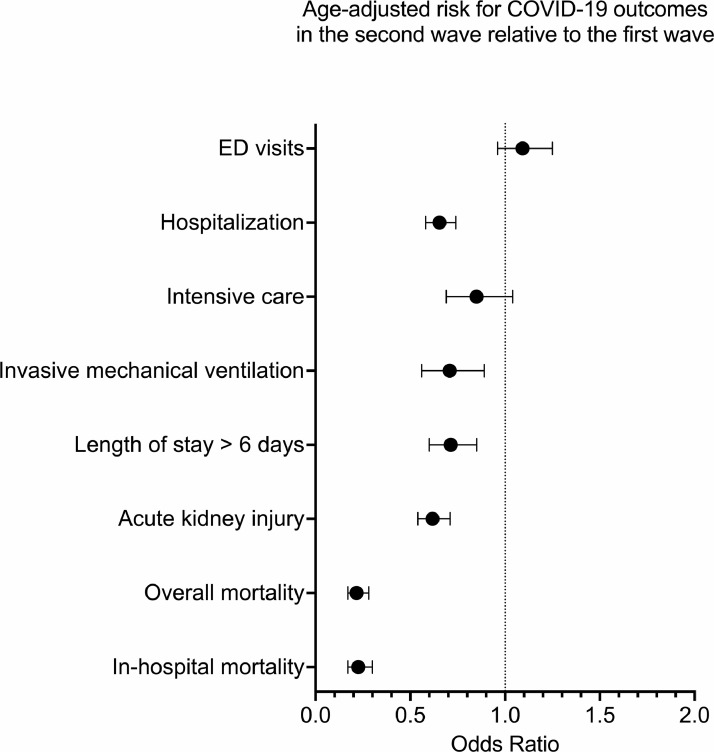
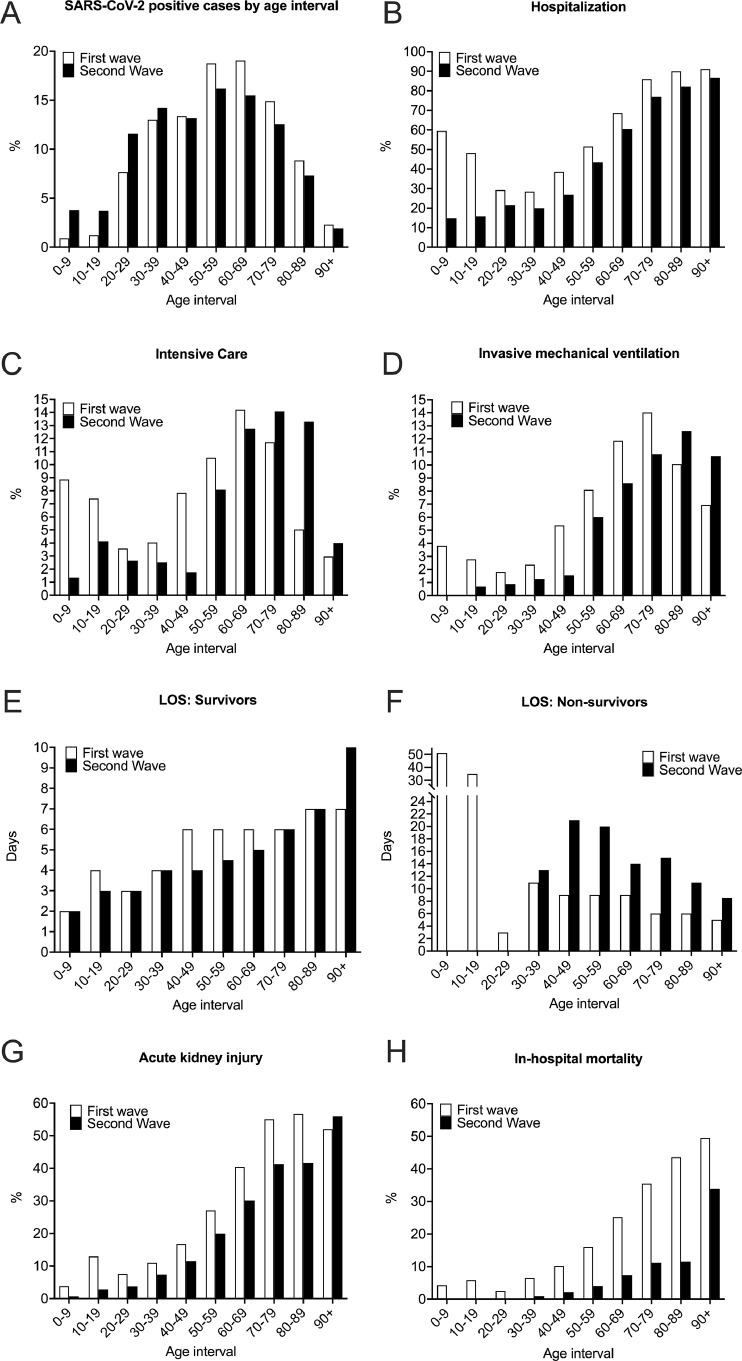
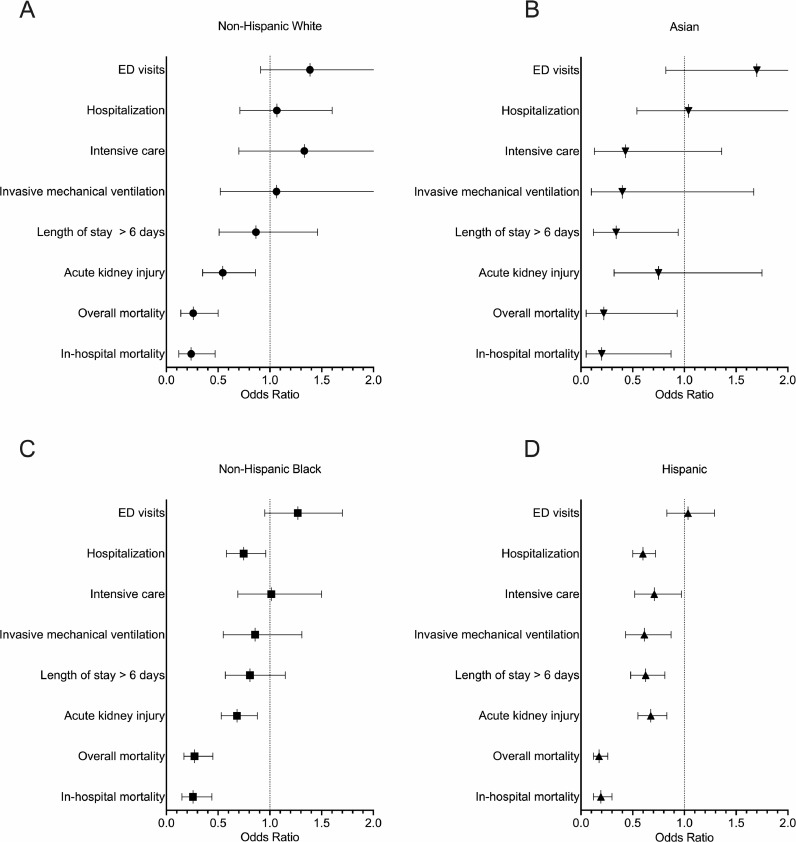
Findings: A total of 122,983 individuals were tested for SARS-CoV-2 infection, of which 12,659 tested positive. The second wave was characterized by a younger demographic, fewer comorbidities, less extreme laboratory values at presentation, and lower risk of adverse outcomes, including in-hospital mortality (adj. OR = 0·23, 99·5% CI = 0·17 to 0·30), hospitalization (adj. OR = 0·65, 99·5% CI = 0·58 to 0·74), invasive mechanical ventilation (adj. OR = 0·70, 99·5% CI = 0·56 to 0·89), acute kidney injury (adj. OR = 0·62, 99·5% CI = 0·54 to 0·71), and length of stay (adj. OR = 0·71, 99·5% CI = 0·60 to 0·85), with Black and Hispanic patients demonstrating most improvement in clinical outcomes.
Interpretation: The second COVID-19 wave in the Bronx exhibits improved clinical outcomes compared to the first wave across all age, racial, and ethnic groups, with minority groups showing more improvement, which is encouraging news in the battle against health disparities.
Keywords: Bronx; COVID-19; Coronavirus; Ethnicity; Mortality; Race; Resurgence; SARS-CoV-2.
© 2021 The Author(s). Published by Elsevier Ltd.
Conflict of interest statement
None.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
