

Association Between Testosterone Treatment and Risk of Incident Cardiovascular Events Among US Male Veterans With Low Testosterone Levels and Multiple Medical Comorbidities
- PMID: 34423650
- PMCID: PMC8649267
- DOI: 10.1161/JAHA.120.020562
Association Between Testosterone Treatment and Risk of Incident Cardiovascular Events Among US Male Veterans With Low Testosterone Levels and Multiple Medical Comorbidities
Abstract
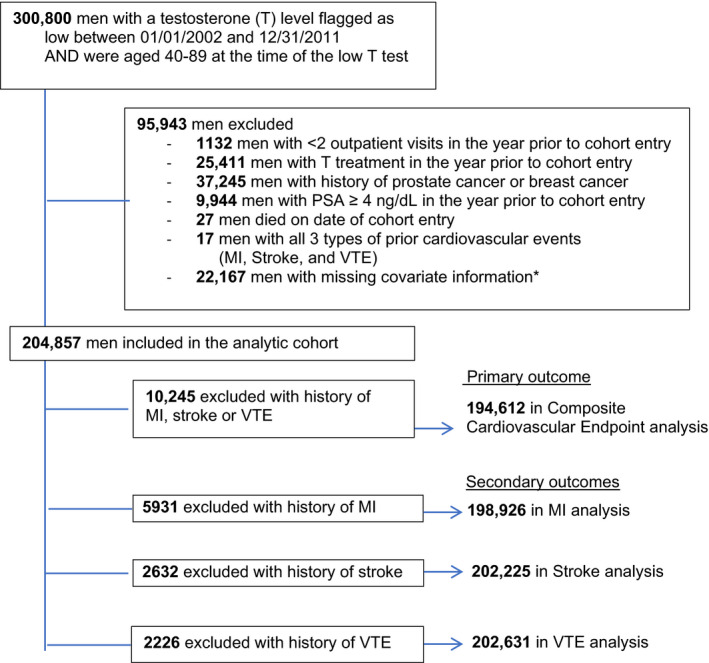
Background Testosterone treatment is common in men, although risks for major cardiovascular events are unclear. Methods and Results A study was conducted in US male veterans, aged ≥40 years, with low serum testosterone and multiple medical comorbidities and without history of myocardial infarction, stroke, venous thromboembolism, prostate cancer, or testosterone treatment in the prior year. For the primary outcome, we examined if testosterone treatment was associated with a composite cardiovascular outcome (incident myocardial infarction, ischemic stroke, or venous thromboembolism). Testosterone use was modeled as intramuscular or transdermal and as current use, former use, and no use. Current testosterone users were compared with former users to reduce confounding by indication. The cohort consisted of 204 857 men with a mean (SD) age of 60.9 (9.9) years and 4.7 (3.5) chronic medical conditions. During follow-up of 4.3 (2.8) years, 12 645 composite cardiovascular events occurred. In adjusted Cox regression analyses, current use of transdermal testosterone was not associated with risk for the composite cardiovascular outcome (hazard ratio [HR], 0.89; 95% CI, 0.76-1.05) in those without prevalent cardiovascular disease, and in those with prevalent cardiovascular disease was associated with lower risk (HR, 0.80; 95% CI, 0.70-0.91). In similar analyses, current use of intramuscular testosterone was not associated with risk for the composite cardiovascular outcome in men without or with prevalent cardiovascular disease (HR, 0.91; 95% CI, 0.80-1.04; HR, 0.98; 95% CI, 0.89-1.09, respectively). Conclusions In a large cohort of men without a history of myocardial infarction, stroke, or venous thromboembolism, testosterone treatment was not associated with increased risk for incident composite cardiovascular events.
Keywords: cohort study; myocardial infarction; stroke; testosterone; thrombosis.
Conflict of interest statement
Dr Walsh is a consultant for Boston Scientific. Dr Matsumoto has obtained research support from AbbVie; is on advisory boards for AbbVie; and is an editor for UpToDate. The remaining authors have no disclosures to report.
Figures
References
-
- Vigen R, O'Donnell CI, Baron AE, Grunwald GK, Maddox TM, Bradley SM, Barqawi A, Woning G, Wierman ME, Plomondon ME, et al. Association of testosterone therapy with mortality, myocardial infarction, and stroke in men with low testosterone levels. JAMA. 2013;310:1829–1836. DOI: 10.1001/jama.2013.280386. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
