

The efficacy and safety of PD-1/PD-L1 immune checkpoint inhibitors in treating advanced urothelial cancer: a meta-analysis of clinical trials
- PMID: 34424218
- PMCID: PMC8436906
- DOI: 10.18632/aging.203429
The efficacy and safety of PD-1/PD-L1 immune checkpoint inhibitors in treating advanced urothelial cancer: a meta-analysis of clinical trials
Abstract
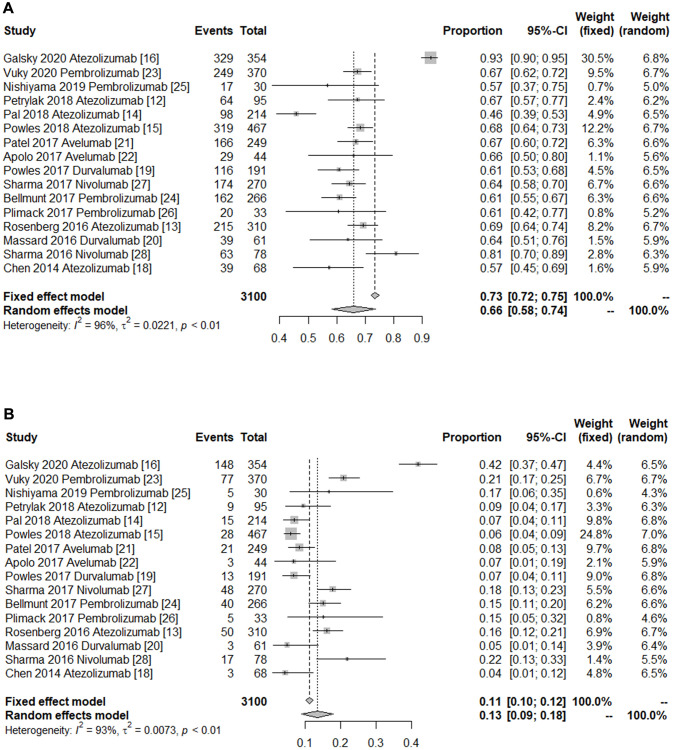
Survival outcomes in advanced urothelial cancer (UC) are dismal. Over the past years, immunotherapy remains an evolving treatment modality for these patients. This meta-analysis was performed to comprehensively evaluate the efficacy and safety of immune checkpoint inhibitors. For this purpose, 18 clinical trials comprising a total of 3,144 patients were identified from the PubMed database up to September 2020. Overall, the objective response rate (ORR) to PD-1/PD-L1 inhibitors was 0.20 [95% confidence intervals (CI) 0.17-0.23]. Furthermore, the pooled 1-year overall survival (OS) and 1-year progression-free survival (PFS) rates were 0.43 (95% CI 0.33-0.53) and 0.19 (95% CI 0.17-0.21), respectively. The summary rates of any-grade and grade ≥3 adverse events (AEs) were 0.66 (95% CI 0.58-0.74) and 0.13 (95% CI 0.09-0.18), respectively. Among the different subgroups, PD-1/PD-L1 inhibitors elicited a promising ORR in patients with lymph node-only metastasis compared to those with visceral metastasis (0.41 VS. 0.17). Additionally, patients with primary tumor in the lower tract had higher ORR compared to those with primary tumor in the upper tract (0.24 VS. 0.15). Briefly speaking, this immunotherapy protocol showed an encouraging efficacy and acceptable safety profile in the treatment of advanced UC. Moreover, our findings provided potential clinical significance for patients with lymph node-only metastasis or primary tumor in the lower tract. However, these exciting findings need further confirmation.
Keywords: efficacy; immunotherapy; meta-analysis; safety; urothelial cancer.
Conflict of interest statement
Figures



References
-
- Cumberbatch MGK, Jubber I, Black PC, Esperto F, Figueroa JD, Kamat AM, Kiemeney L, Lotan Y, Pang K, Silverman DT, Znaor A, Catto JWF. Epidemiology of Bladder Cancer: A Systematic Review and Contemporary Update of Risk Factors in 2018. Eur Urol. 2018; 74:784–95. 10.1016/j.eururo.2018.09.001 - DOI - PubMed
-
- Witjes JA, Bruins HM, Cathomas R, Compérat EM, Cowan NC, Gakis G, Hernández V, Linares Espinós E, Lorch A, Neuzillet Y, Rouanne M, Thalmann GN, Veskimäe E, et al.. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur Urol. 2021; 79:82–104. 10.1016/j.eururo.2020.03.055 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
