

Intracranial aneurysm wall enhancement as an indicator of instability: a systematic review and meta-analysis
- PMID: 34424585
- PMCID: PMC9292155
- DOI: 10.1111/ene.15046
Intracranial aneurysm wall enhancement as an indicator of instability: a systematic review and meta-analysis
Abstract
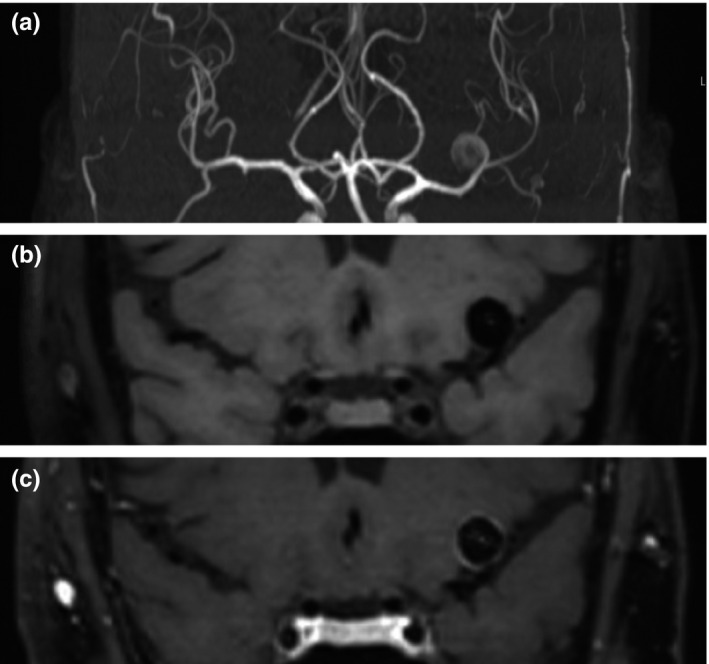
Background and purpose: Aneurysm wall enhancement (AWE) of intracranial aneurysms on magnetic resonance imaging has been described in previous studies as a surrogate marker of instability. With this study, an updated literature overview and summary risk estimates of the association between AWE and different specific outcomes (i.e., rupture, growth or symptomatic presentation) for both cross-sectional and longitudinal studies are provided.
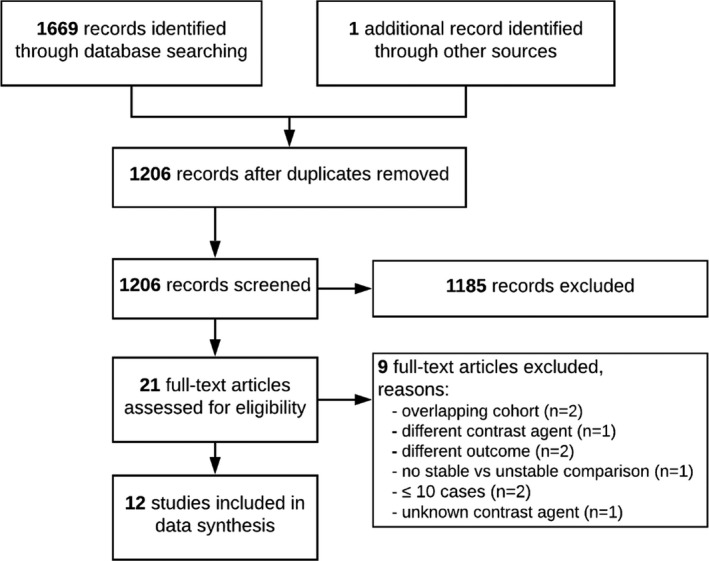
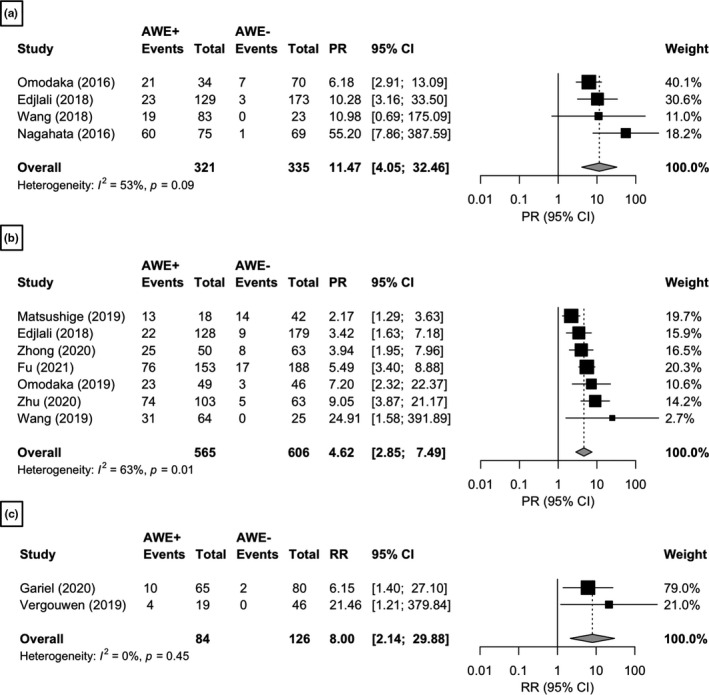
Methods: The PRISMA guideline was followed and a search was performed of PubMed and Embase to 1 January 2021 for studies that reported on AWE and aneurysm instability. In cross-sectional studies, AWE was compared between patients with stable and unstable aneurysms. In longitudinal studies, AWE of stable aneurysms was assessed at baseline after which patients were followed longitudinally. Risk ratios were calculated for longitudinal studies, prevalence ratios for cross-sectional studies and then the ratios were pooled in a random-effects meta-analysis. Also, the performance of AWE to differentiate between stable and unstable aneurysms was evaluated.
Results: Twelve studies were included with a total of 1761 aneurysms. In cross-sectional studies, AWE was positively associated with rupture (prevalence ratio 11.47, 95% confidence interval [CI] 4.05-32.46) and growth or symptomatic presentation (prevalence ratio 4.62, 95% CI 2.85-7.49). Longitudinal studies demonstrated a positive association between AWE and growth or rupture (risk ratio 8.00, 95% CI 2.14-29.88). Assessment of the performance of AWE showed high sensitivities, mixed specificities, low positive predictive values and high negative predictive values.
Conclusions: Although AWE is positively associated with aneurysm instability, current evidence mostly supports the use of its absence as a surrogate marker of aneurysm stability.
Keywords: aneurysm; gadolinium; inflammation; magnetic resonance angiography; risk assessment.
© 2021 The Authors. European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
None.
Figures
Comment in
-
Wall enhancement as an emerging marker of intracranial aneurysm stability: Roadmap toward a potential target for clinical trials.Eur J Neurol. 2021 Nov;28(11):3550-3551. doi: 10.1111/ene.15094. Epub 2021 Sep 12. Eur J Neurol. 2021. PMID: 34478593 No abstract available.
References
-
- Rinkel GJE, Algra A. Long‐term outcomes of patients with aneurysmal subarachnoid haemorrhage. Lancet Neurol. 2011;10:349‐356. - PubMed
-
- Lee WK, Oh CW, Lee H, Lee KS, Park H. Factors influencing the incidence and treatment of intracranial aneurysm and subarachnoid hemorrhage: time trends and socioeconomic disparities under a universal healthcare system. J Neurointerv Surg. 2019;11:159‐165. - PubMed
-
- Thompson BG, Brown RD, Amin‐Hanjani S, et al. Guidelines for the management of patients with unruptured intracranial aneurysms: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2015;46:2368‐2400. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
