

Organized primary human papillomavirus-based cervical screening: A randomized healthcare policy trial
- PMID: 34424907
- PMCID: PMC8423359
- DOI: 10.1371/journal.pmed.1003748
Organized primary human papillomavirus-based cervical screening: A randomized healthcare policy trial
Abstract
Background: Clinical trials in the research setting have demonstrated that primary human papillomavirus (HPV)-based screening results in greater protection against cervical cancer compared with cytology, but evidence from real-life implementation was missing. To evaluate the effectiveness of HPV-based cervical screening within a real-life screening program, the organized, population-based cervical screening program in the capital region of Sweden offered either HPV- or cytology-based screening in a randomized manner through a randomized healthcare policy (RHP).
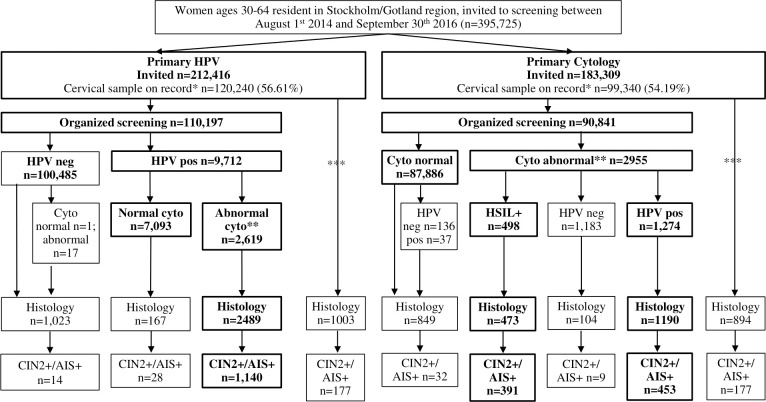
Methods and findings: A total of 395,725 women aged 30 to 64 years that were invited for their routine cervical screening visit were randomized without blinding to either cytology-based screening with HPV triage (n = 183,309) or HPV-based screening, with cytology triage (n = 212,416 women) between September 1, 2014 and September 30, 2016 and follow-up through June 30, 2017. The main outcome was non-inferior detection rate of cervical intraepithelial neoplasia grade 2 or worse (CIN2+). Secondary outcomes included superiority in CIN2+ detection, screening attendance, and referral to histology. In total, 120,240 had a cervical screening sample on record in the study period in the HPV arm and 99,340 in the cytology arm and were followed for the outcomes of interest. In per-protocol (PP) analyses, the detection rate of CIN2+ was 1.03% (95% confidence interval (CI) 0.98 to 1.10) in the HPV arm and 0.93% (0.87 to 0.99) in the cytology arm (p for non-inferiority <0.0001; odds ratio (OR) 1.11 (95% CI 1.02 to 1.22)). There were 46 cervical cancers detected in the HPV arm (0.04% (0.03 to 0.06)) and 48 cancers detected in the cytology arm (0.05% (0.04 to 0.07)) (p for non-inferiority <0.0001; OR 0.79 (0.53 to 1.18)). Intention-to-screen (ITS) analyses found few differences. In the HPV arm, there was a modestly increased attendance after new invitations (68.56% (68.31 to 68.80) vs. 67.71% (67.43 to 67.98); OR 1.02 (1.00 to 1.03)) and increased rate of referral with completed biopsy (3.89% (3.79 to 4.00) vs. 3.53% (3.42 to 3.65); OR 1.10 (1.05 to 1.15)). The main limitations of this analysis are that only the baseline results are presented, and there was an imbalance in invitations between the study arms.
Conclusions: In this study, we observed that a real-life RHP of primary HPV-based screening was acceptable and effective when evaluated against cytology-based screening, as indicated by comparable participation, referral, and detection rates.
Trial registration: ClinicalTrials.gov NCT01511328.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization. Comprehensive cervical cancer control: a guide to essential practice. 2nd ed. Geneva, Switzerland: World Health Organization; 2014. - PubMed
-
- International Agency for Research on Cancer. IARC monographs on the evaluation of carcinogenic risks to humans, vol 100b, Human Papillomaviruses. Lyon, France: International Agency for Research on Cancer; 2012.
-
- von Karsa L, Arbyn M, De Vuyst H, Dillner J, Dillner L, Franceschi S, et al. European guidelines for quality assurance in cervical cancer screening. Summary of the supplements on HPV screening and vaccination. Papillomavirus Res. 2015;1:22–31.
-
- Arbyn M, Anttila A, Jordan J, Ronco G, Schenck U, Segnan N, et al. European Guidelines for Quality Assurance in Cervical Cancer Screening. 2nd ed. Luxembourg: Office for Official Publications of the European Communities; 2008.
