

Awake prone positioning for COVID-19 acute hypoxaemic respiratory failure: a randomised, controlled, multinational, open-label meta-trial
- PMID: 34425070
- PMCID: PMC8378833
- DOI: 10.1016/S2213-2600(21)00356-8
Awake prone positioning for COVID-19 acute hypoxaemic respiratory failure: a randomised, controlled, multinational, open-label meta-trial
Abstract
Background: Awake prone positioning has been reported to improve oxygenation for patients with COVID-19 in retrospective and observational studies, but whether it improves patient-centred outcomes is unknown. We aimed to evaluate the efficacy of awake prone positioning to prevent intubation or death in patients with severe COVID-19 in a large-scale randomised trial.
Methods: In this prospective, a priori set up and defined, collaborative meta-trial of six randomised controlled open-label superiority trials, adults who required respiratory support with high-flow nasal cannula for acute hypoxaemic respiratory failure due to COVID-19 were randomly assigned to awake prone positioning or standard care. Hospitals from six countries were involved: Canada, France, Ireland, Mexico, USA, Spain. Patients or their care providers were not masked to allocated treatment. The primary composite outcome was treatment failure, defined as the proportion of patients intubated or dying within 28 days of enrolment. The six trials are registered with ClinicalTrials.gov, NCT04325906, NCT04347941, NCT04358939, NCT04395144, NCT04391140, and NCT04477655.
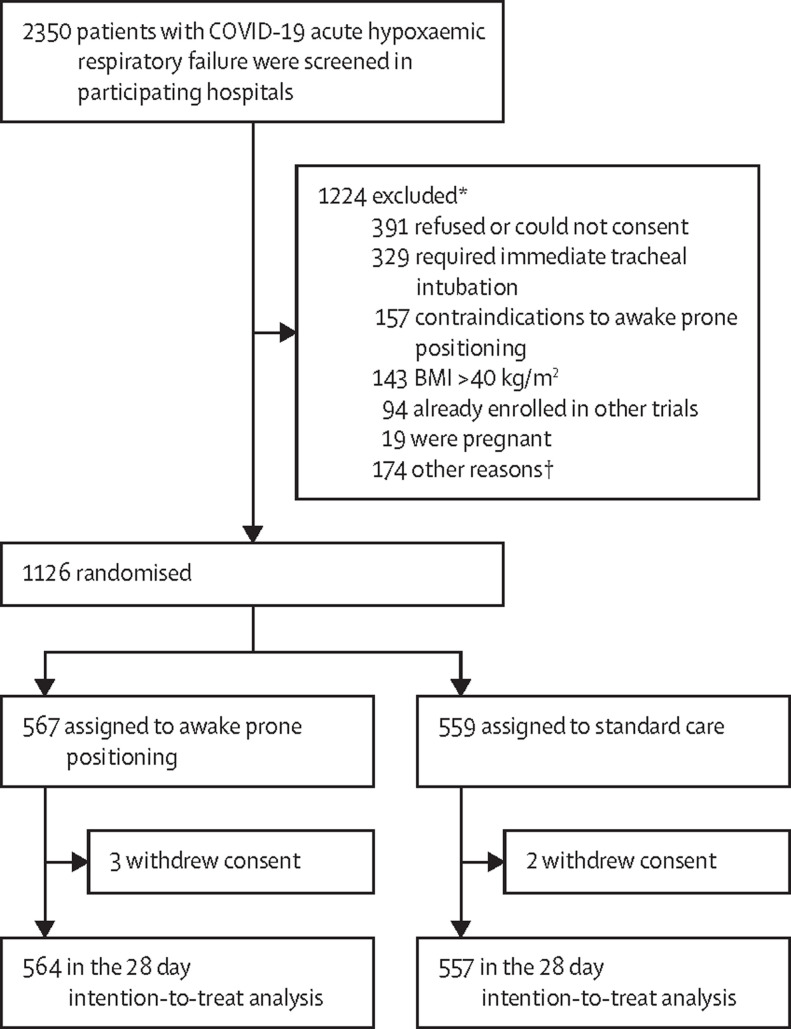
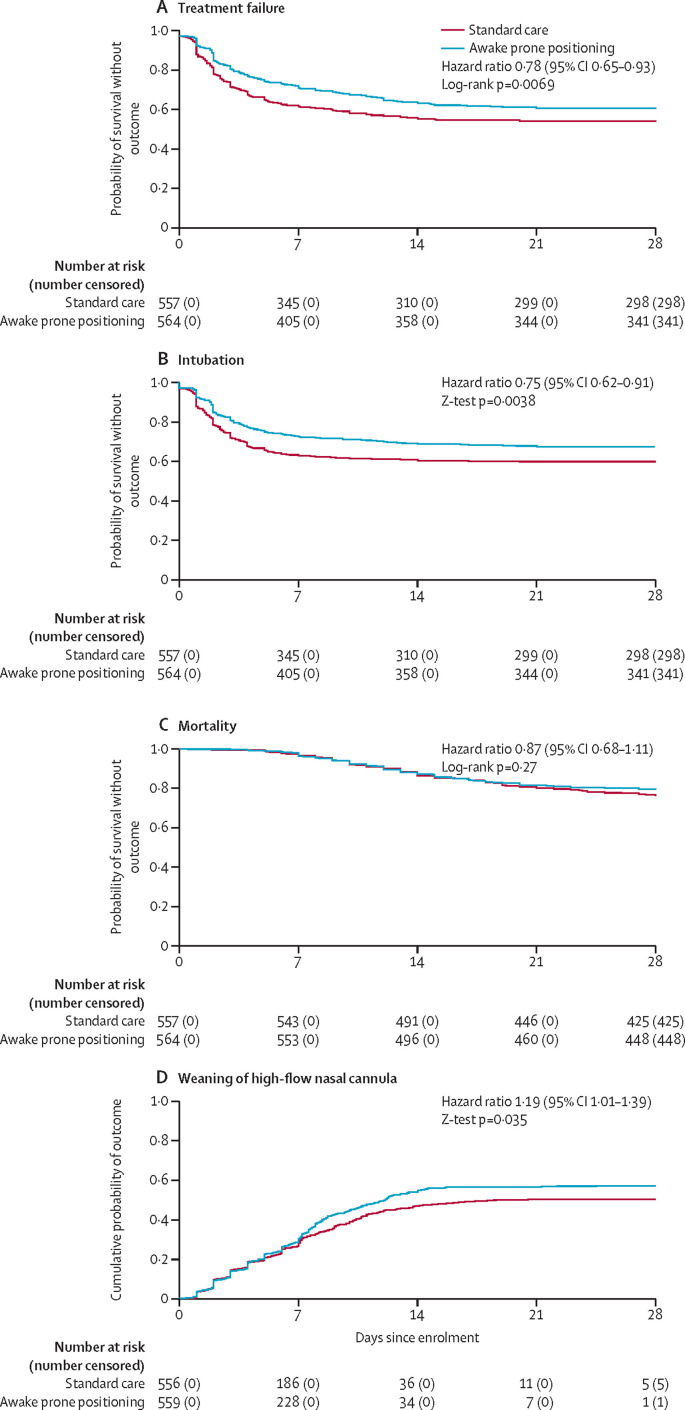
Findings: Between April 2, 2020 and Jan 26, 2021, 1126 patients were enrolled and randomly assigned to awake prone positioning (n=567) or standard care (n=559). 1121 patients (excluding five who withdrew from the study) were included in the intention-to-treat analysis. Treatment failure occurred in 223 (40%) of 564 patients assigned to awake prone positioning and in 257 (46%) of 557 patients assigned to standard care (relative risk 0·86 [95% CI 0·75-0·98]). The hazard ratio (HR) for intubation was 0·75 (0·62-0·91), and the HR for mortality was 0·87 (0·68-1·11) with awake prone positioning compared with standard care within 28 days of enrolment. The incidence of prespecified adverse events was low and similar in both groups.
Interpretation: Awake prone positioning of patients with hypoxaemic respiratory failure due to COVID-19 reduces the incidence of treatment failure and the need for intubation without any signal of harm. These results support routine awake prone positioning of patients with COVID-19 who require support with high-flow nasal cannula.
Funding: Open AI inc, Rice Foundation, Projet Hospitalier de Recherche Clinique Interrégional, Appel d'Offre 2020, Groupement Interrégional de Recherche Clinique et d'Innovation Grand Ouest, Association pour la Promotion à Tours de la Réanimation Médicale, Fond de dotation du CHRU de Tours, Fisher & Paykel Healthcare Ltd.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests SE discloses consultancies from Aerogen Ltd, research support from Aerogen Ltd, Fisher & Paykel Healthcare Ltd, Hamilton medical, travel reimbursements from Aerogen Ltd and Fisher & Paykel Healthcare Ltd. JL discloses research funding from Fisher & Paykel Healthcare Ltd, Aerogen Ltd, and Rice Foundation, and speaker fees from AARC and Fisher & Paykel Healthcare Ltd. IP discloses a research grant and speaker fees from Fisher & Paykel Healthcare Ltd. YP discloses research support from Fisher & Paykel Healthcare Ltd. OR discloses a research grant from Hamilton Medical and speaker fees from Hamilton Medical, Ambu and Aerogen Ltd, and non-financial research support from Timpel and Masimo Corporation. His institution received fees for consultancy from Hamilton Medical. DV discloses research funding from Teleflex Medical, Inc and Rice Foundation, and speaker fees from Theravance Biopharma. MWT discloses consulting fees from Fisher and Paykel. JRM discloses research support from Fisher & Paykel, and speaker fees from Fisher & Paykel, Gilead, Dextro, and Linet. JGL discloses consulting fees from Baxter Healthcare and Glaxosmithkline. All other authors have no competing interests to disclose.
Figures
Comment in
-
Awake prone positioning in COVID-19: is tummy time ready for prime time?Lancet Respir Med. 2021 Dec;9(12):1347-1349. doi: 10.1016/S2213-2600(21)00368-4. Epub 2021 Aug 20. Lancet Respir Med. 2021. PMID: 34425072 Free PMC article. No abstract available.
-
Prone positioning might reduce the need for intubation in people with severe COVID-19.Lancet Respir Med. 2021 Dec;9(12):e110. doi: 10.1016/S2213-2600(21)00437-9. Lancet Respir Med. 2021. PMID: 34861159 Free PMC article. No abstract available.
-
Awake prone positioning for COVID-19 acute respiratory failure: imaging and histological background.Lancet Respir Med. 2022 Feb;10(2):e14. doi: 10.1016/S2213-2600(21)00554-3. Lancet Respir Med. 2022. PMID: 35120610 Free PMC article. No abstract available.
References
-
- Intensive care national audit and research centre ICNARC report on COVID-19 in critical care: England, Wales and Northern Ireland. 2021. https://www.icnarc.org/DataServices/Attachments/Download/2d288f8e-728e-e...
-
- Berlin DA, Gulick RM, Martinez FJ. Severe COVID-19. N Engl J Med. 2020;383:2451–2460. - PubMed
-
- Guérin C, Reignier J, Richard J-C, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368:2159–2168. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
