

Problem-solving training as an active ingredient of treatment for youth depression: a scoping review and exploratory meta-analysis
- PMID: 34425770
- PMCID: PMC8383463
- DOI: 10.1186/s12888-021-03260-9
Problem-solving training as an active ingredient of treatment for youth depression: a scoping review and exploratory meta-analysis
Abstract
Background: Problem-solving training is a common ingredient of evidence-based therapies for youth depression and has shown effectiveness as a versatile stand-alone intervention in adults. This scoping review provided a first overview of the evidence supporting problem solving as a mechanism for treating depression in youth aged 14 to 24 years.
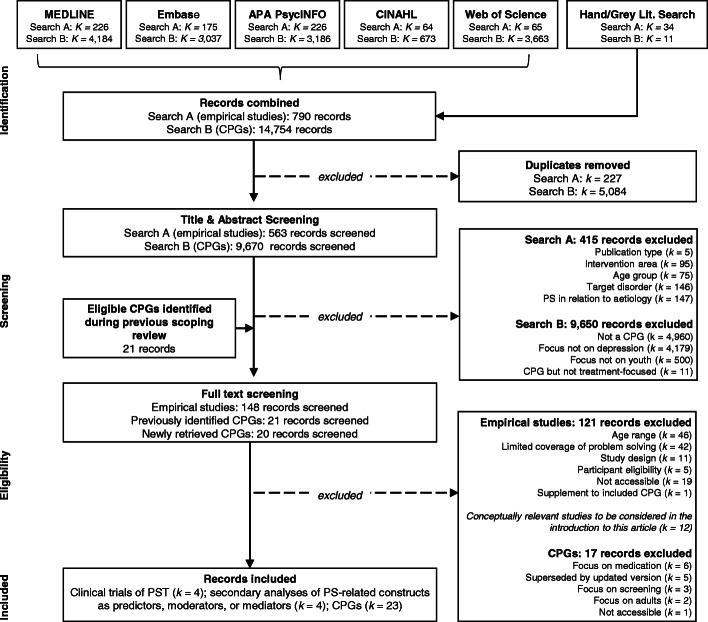
Methods: Five bibliographic databases (APA PsycINFO, CINAHL, Embase, MEDLINE, Web of Science) and the grey literature were systematically searched for controlled trials of stand-alone problem-solving therapy; secondary analyses of trial data exploring problem-solving-related concepts as predictors, moderators, or mediators of treatment response within broader therapies; and clinical practice guidelines for youth depression. Following the scoping review, an exploratory meta-analysis examined the overall effectiveness of stand-alone problem-solving therapy.
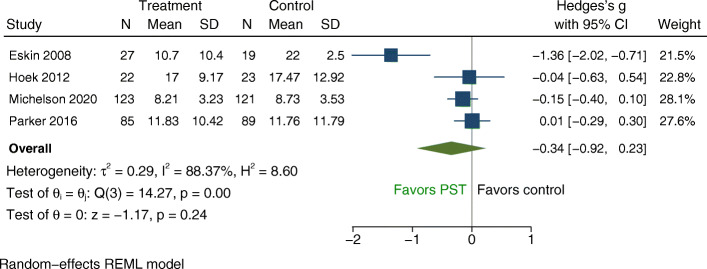
Results: Inclusion criteria were met by four randomized trials of problem-solving therapy (524 participants); four secondary analyses of problem-solving-related concepts as predictors, moderators, or mediators; and 23 practice guidelines. The only clinical trial rated as having a low risk of bias found problem-solving training helped youth solve personal problems but was not significantly more effective than the control at reducing emotional symptoms. An exploratory meta-analysis showed a small and non-significant effect on self-reported depression or emotional symptoms (Hedges' g = - 0.34; 95% CI: - 0.92 to 0.23) with high heterogeneity. Removing one study at high risk of bias led to a decrease in effect size and heterogeneity (g = - 0.08; 95% CI: - 0.26 to 0.10). A GRADE appraisal suggested a low overall quality of the evidence. Tentative evidence from secondary analyses suggested problem-solving training might enhance outcomes in cognitive-behavioural therapy and family therapy, but dedicated dismantling studies are needed to corroborate these findings. Clinical practice guidelines did not recommend problem-solving training as a stand-alone treatment for youth depression, but five mentioned it as a treatment ingredient.
Conclusions: On its own, problem-solving training may be beneficial for helping youth solve personal challenges, but it may not measurably reduce depressive symptoms. Youth experiencing elevated depressive symptoms may require more comprehensive psychotherapeutic support alongside problem-solving training. High-quality studies are needed to examine the effectiveness of problem-solving training as a stand-alone approach and as a treatment ingredient.
Keywords: Active ingredient; Adolescence; Depression; Problem solving; Youth.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Comment in
-
Young people's mental health is finally getting the attention it needs.Nature. 2021 Oct;598(7880):235-236. doi: 10.1038/d41586-021-02690-5. Nature. 2021. PMID: 34621038 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
