

Consistency of associations of systolic and diastolic blood pressure with white matter hyperintensities: A meta-analysis
- PMID: 34427478
- PMCID: PMC8864334
- DOI: 10.1177/17474930211043364
Consistency of associations of systolic and diastolic blood pressure with white matter hyperintensities: A meta-analysis
Abstract
Background: White matter hyperintensities are the commonest manifestation of cerebral small vessel disease, associated with stroke, functional impairment, and cognitive decline. They are commonly preceded by hypertension, but the magnitude and clinical importance of this association is unclear.
Aims: Quantify the relationship between blood pressure and white matter hyperintensities across studies.
Methods: PubMed and EMBASE were searched for studies reporting associations between concurrent or historic blood pressure and white matter hyperintensities. Beta coefficients from linear models were extracted, whether standardized, unstandardized, unadjusted or adjusted for age, sex, and cardiovascular risk factors. Beta-coefficients were combined by fixed and random effects meta-analysis, combining standardized beta-coefficients or unstandardized coefficients measured by consistent methods.
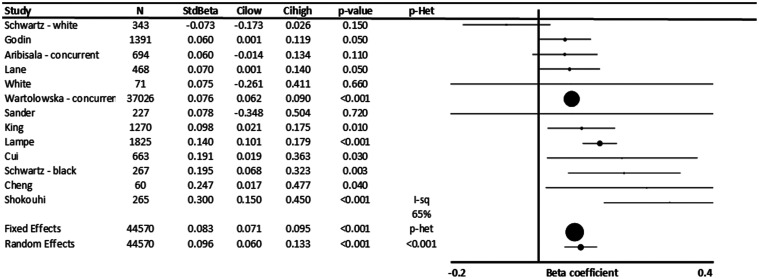
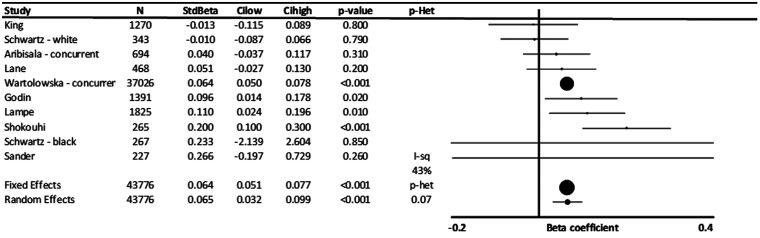
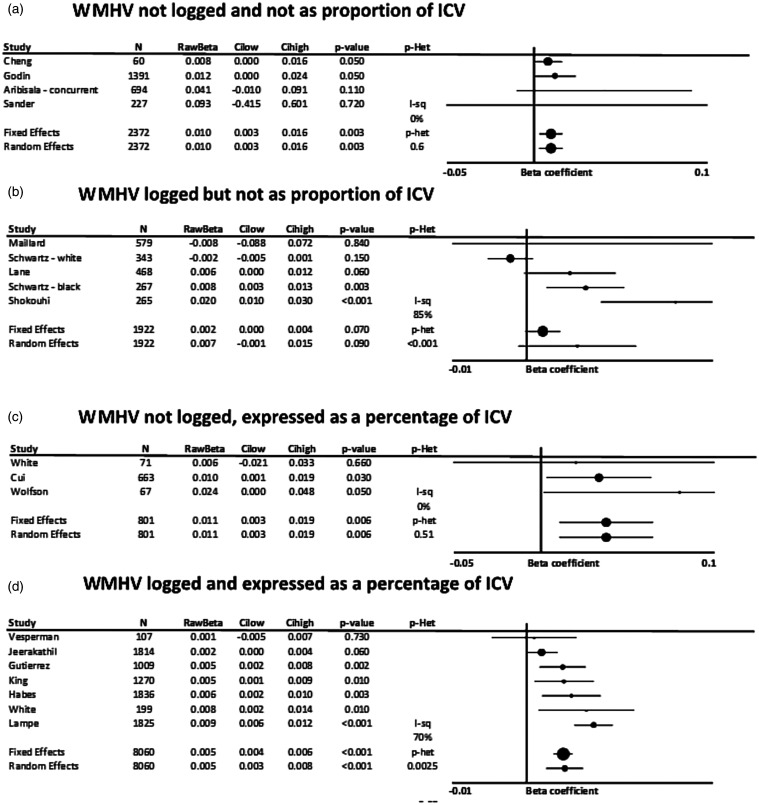
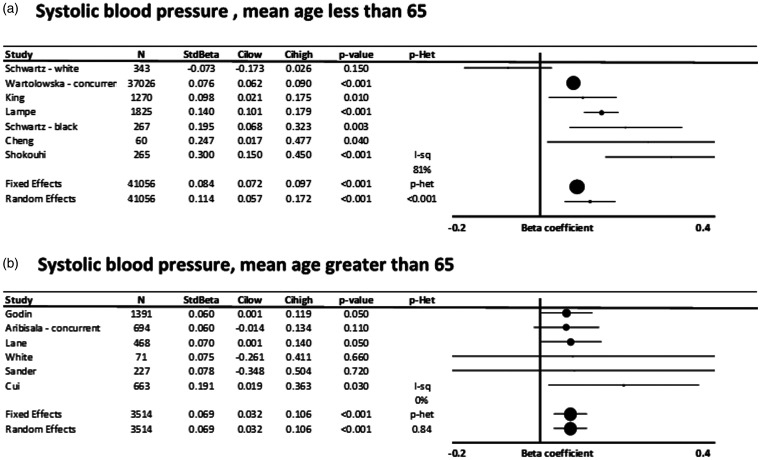
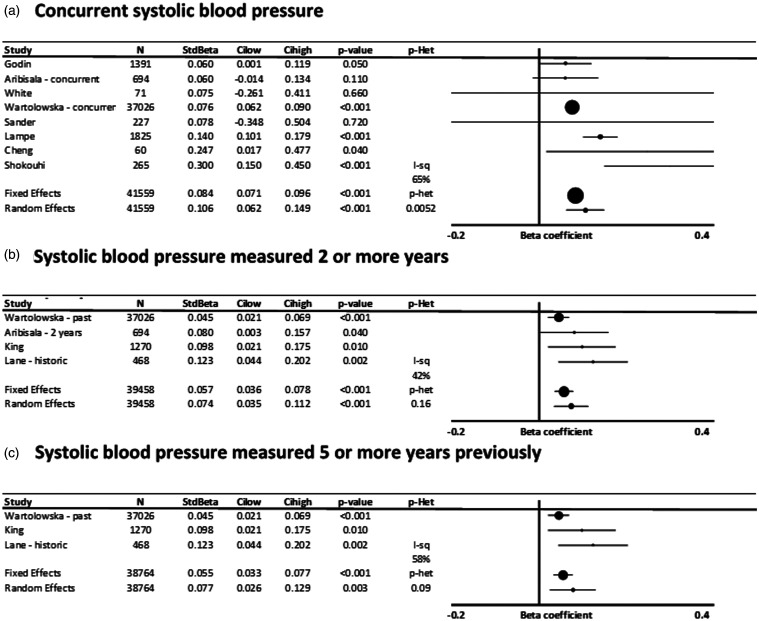
Results: Twenty-five of 3230 papers were eligible, including 53,392 participants. Systolic blood pressure was significantly associated with white matter hyperintensity volume (WMHV) after maximal adjustment (standardized beta 0.096, 95%CI 0.06-0.133, p < 0.001, I2 = 65%), including for concurrent readings (b = 0.106, p < 0.001) or readings five years previously (b = 0.077, p < 0.001), and for younger or older populations (mean age < 65: b = 0.114; >65 b = 0.069). Unstandardized, adjusted associations were similar for raw WMHV, log-transformed WMHV, or WMHV as percentage of intracranial volume. Unadjusted associations with systolic blood pressure (SBP) were greater (standardized beta = 0.273, 0.262-0.284, p < 0.0001). However, while associations with DBP were weaker than SBP (standardized beta = 0.065, p < 0.001), they were minimally affected by adjustment for age.
Conclusions: A standard deviation increase in SBP is associated with 10% of a standard deviation increase in WMHV, providing the current best estimate of the potential reduction in progression of white matter hyperintensities expected with good control of blood pressure.
Keywords: Hypertension; blood pressure; meta-analysis; white matter hyperintensities.
Conflict of interest statement
Figures
References
-
- Teodorczuk A, Firbank MJ, Pantoni L, et al. Group L. Relationship between baseline white-matter changes and development of late-life depressive symptoms: 3-year results from the LADIS study. Psychol Med 2010; 40: 603–610. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
