

Rates of Influenza-Associated Hospitalization, Intensive Care Unit Admission, and In-Hospital Death by Race and Ethnicity in the United States From 2009 to 2019
- PMID: 34427679
- PMCID: PMC8385599
- DOI: 10.1001/jamanetworkopen.2021.21880
Rates of Influenza-Associated Hospitalization, Intensive Care Unit Admission, and In-Hospital Death by Race and Ethnicity in the United States From 2009 to 2019
Abstract
Importance: Racial and ethnic minority groups, such as Black, Hispanic, American Indian or Alaska Native, and Asian or Pacific Islander persons, often experience higher rates of severe influenza disease.
Objective: To describe rates of influenza-associated hospitalization, intensive care unit (ICU) admission, and in-hospital death by race and ethnicity over 10 influenza seasons.
Design, setting, and participants: This cross-sectional study used data from the Influenza-Associated Hospitalization Surveillance Network (FluSurv-NET), which conducts population-based surveillance for laboratory-confirmed influenza-associated hospitalizations in selected counties, representing approximately 9% of the US population. Influenza hospitalizations from the 2009 to 2010 season to the 2018 to 2019 season were analyzed. Data were analyzed from October 2020 to July 2021.
Main outcomes and measures: The main outcomes were age-adjusted and age-stratified rates of influenza-associated hospitalization, ICU admission, and in-hospital death by race and ethnicity overall and by influenza season.
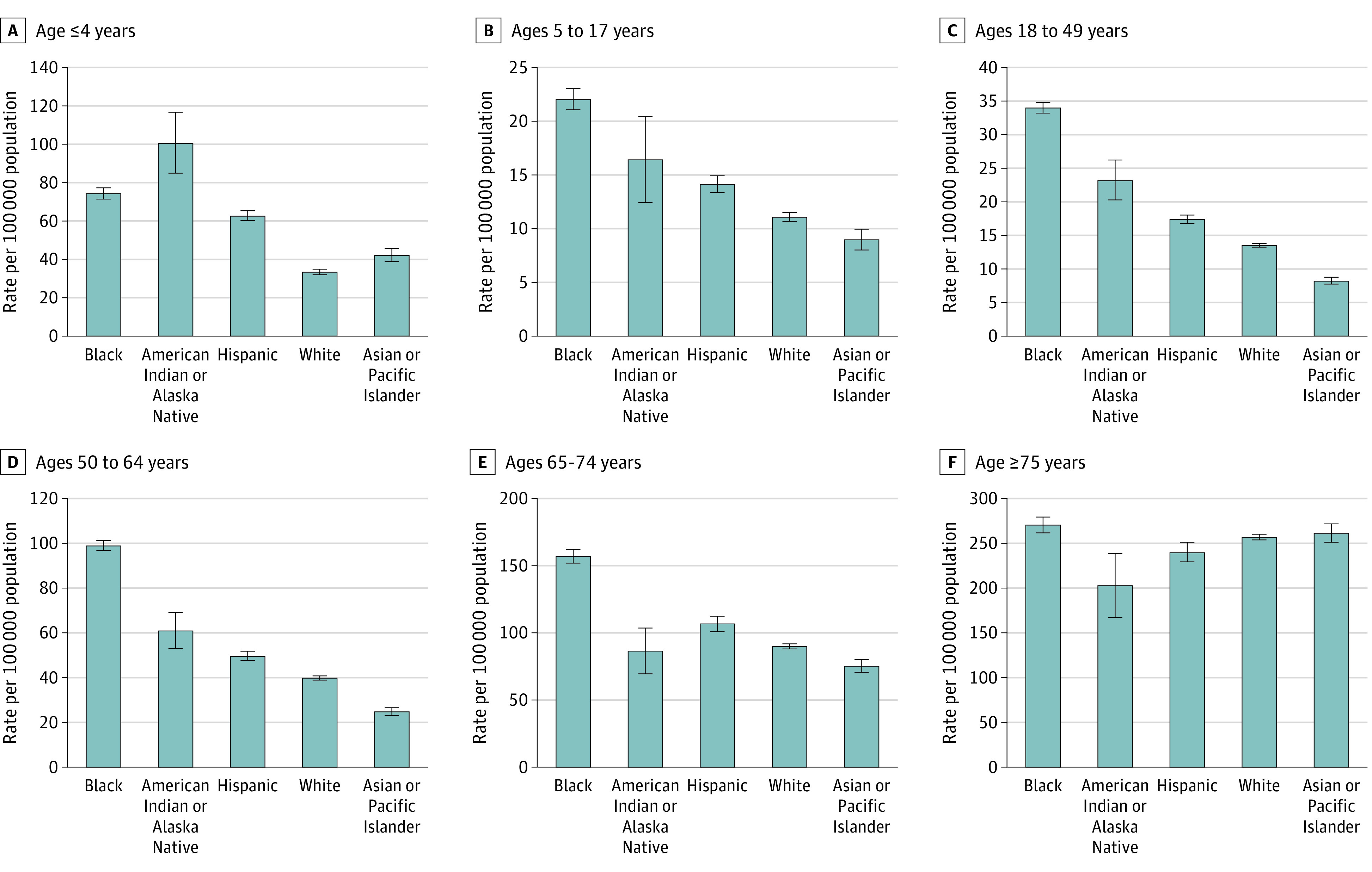
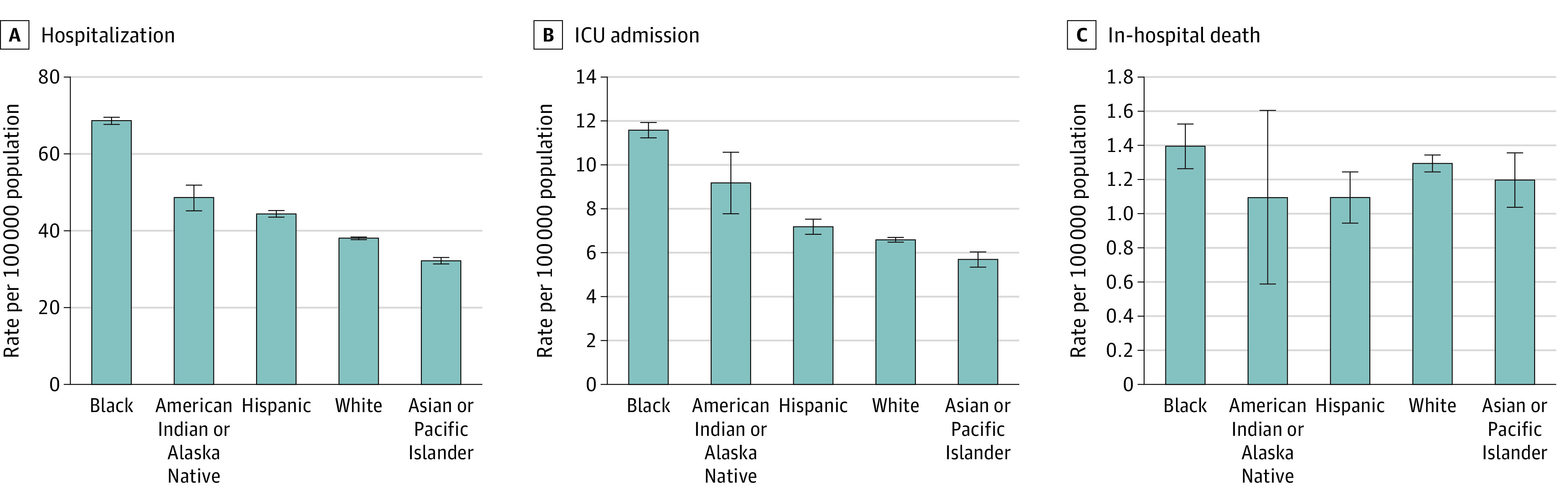
Results: Among 113 352 persons with an influenza-associated hospitalization (34 436 persons [32.0%] aged ≥75 years; 61 009 [53.8%] women), 70 225 persons (62.3%) were non-Hispanic White (White), 24 850 persons (21.6%) were non-Hispanic Black (Black), 11 903 persons (10.3%) were Hispanic, 5517 persons (5.1%) were non-Hispanic Asian or Pacific Islander, and 857 persons (0.7%) were non-Hispanic American Indian or Alaska Native. Among persons aged younger than 75 years and compared with White persons of the same ages, Black persons were more likely to be hospitalized (eg, age 50-64 years: rate ratio [RR], 2.50 95% CI, 2.43-2.57) and to be admitted to an ICU (eg, age 50-64 years: RR, 2.09; 95% CI, 1.96-2.23). Among persons aged younger than 50 years and compared with White persons of the same ages, American Indian or Alaska Native persons were more likely to be hospitalized (eg, age 18-49 years: RR, 1.72; 95% CI, 1.51-1.96) and to be admitted to an ICU (eg, age 18-49 years: RR, 1.84; 95% CI, 1.40-2.42). Among children aged 4 years or younger and compared with White children, hospitalization rates were higher in Black children (RR, 2.21; 95% CI, 2.10-2.33), Hispanic children (RR, 1.87; 95% CI, 1.77-1.97), American Indian or Alaska Native children (RR, 3.00; 95% CI, 2.55-3.53), and Asian or Pacific Islander children (RR, 1.26; 95% CI, 1.16-1.38), as were rates of ICU admission (Black children: RR, 2.74; 95% CI, 2.43-3.09; Hispanic children: RR, 1.96; 95% CI, 1.73-2.23; American Indian and Alaska Native children: RR, 3.51; 95% CI, 2.45-5.05). In this age group and compared with White children, in-hospital death rates were higher among Hispanic children (RR, 2.98; 95% CI, 1.23-7.19), Black children (RR, 3.39; 95% CI, 1.40-8.18), and Asian or Pacific Islander children (RR, 4.35; 95% CI, 1.55-12.22). Few differences were observed in rates of severe influenza-associated outcomes by race and ethnicity among adults aged 75 years or older. For example, in this age group, compared with White adults, hospitalization rates were slightly higher only among Black adults (RR, 1.05; 95% CI 1.02-1.09). Overall, Black persons had the highest age-adjusted hospitalization rate (68.8 [95% CI, 68.0-69.7] hospitalizations per 100 000 population) and ICU admission rate (11.6 [95% CI, 11.2-11.9] admissions per 100 000 population).
Conclusions and relevance: This cross-sectional study found racial and ethnic disparities in rates of severe influenza-associated disease. These data identified subgroups for whom improvements in influenza prevention efforts could be targeted.
Conflict of interest statement
Figures
Similar articles
-
Laboratory-Confirmed Influenza-Associated Hospitalizations Among Children and Adults - Influenza Hospitalization Surveillance Network, United States, 2010-2023.MMWR Surveill Summ. 2024 Oct 31;73(6):1-18. doi: 10.15585/mmwr.ss7706a1. MMWR Surveill Summ. 2024. PMID: 39471107 Free PMC article.
-
Racial and Ethnic Disparities in Rates of COVID-19-Associated Hospitalization, Intensive Care Unit Admission, and In-Hospital Death in the United States From March 2020 to February 2021.JAMA Netw Open. 2021 Oct 1;4(10):e2130479. doi: 10.1001/jamanetworkopen.2021.30479. JAMA Netw Open. 2021. PMID: 34673962 Free PMC article.
-
Vaccination Status and Trends in Adult Coronavirus Disease 2019-Associated Hospitalizations by Race and Ethnicity: March 2020-August 2022.Clin Infect Dis. 2023 Sep 18;77(6):827-838. doi: 10.1093/cid/ciad266. Clin Infect Dis. 2023. PMID: 37132204 Free PMC article.
-
Race and Ethnicity Representation in Phase 2/3 Oncology Clinical Trial Publications: A Systematic Review.JAMA Health Forum. 2024 Jun 7;5(6):e241388. doi: 10.1001/jamahealthforum.2024.1388. JAMA Health Forum. 2024. PMID: 38848090 Free PMC article.
-
Assessment of the Inclusion of Racial/Ethnic Minority, Female, and Older Individuals in Vaccine Clinical Trials.JAMA Netw Open. 2021 Feb 1;4(2):e2037640. doi: 10.1001/jamanetworkopen.2020.37640. JAMA Netw Open. 2021. PMID: 33606033 Free PMC article. Review.
Cited by
-
Risk factor associations for severe COVID-19, influenza and pneumonia in people with diabetes to inform future pandemic preparations: UK population-based cohort study.BMJ Open. 2024 Jan 31;14(1):e078135. doi: 10.1136/bmjopen-2023-078135. BMJ Open. 2024. PMID: 38296292 Free PMC article.
-
Roles and Mechanisms of NLRP3 in Influenza Viral Infection.Viruses. 2023 Jun 8;15(6):1339. doi: 10.3390/v15061339. Viruses. 2023. PMID: 37376638 Free PMC article. Review.
-
Laboratory-Confirmed Influenza-Associated Hospitalizations Among Children and Adults - Influenza Hospitalization Surveillance Network, United States, 2010-2023.MMWR Surveill Summ. 2024 Oct 31;73(6):1-18. doi: 10.15585/mmwr.ss7706a1. MMWR Surveill Summ. 2024. PMID: 39471107 Free PMC article.
-
Identification and characterisation of clinically distinct subgroups of adults hospitalised with influenza in the USA: a repeated cross-sectional study.EClinicalMedicine. 2025 Apr 18;83:103207. doi: 10.1016/j.eclinm.2025.103207. eCollection 2025 May. EClinicalMedicine. 2025. PMID: 40291348 Free PMC article.
-
Advancing health equity through action in antimicrobial stewardship and healthcare epidemiology.Infect Control Hosp Epidemiol. 2024 Apr;45(4):412-419. doi: 10.1017/ice.2024.7. Epub 2024 Feb 14. Infect Control Hosp Epidemiol. 2024. PMID: 38351853 Free PMC article. No abstract available.
References
-
- Centers for Disease Control and Prevention . Disease burden of influenza. Accessed June 9, 2021. https://www.cdc.gov/flu/about/burden/index.html
-
- Moore JT, Ricaldi JN, Rose CE, et al. ; COVID-19 State, Tribal, Local, and Territorial Response Team . Disparities in incidence of COVID-19 among underrepresented racial/ethnic groups in counties identified as hotspots during June 5-18, 2020—22 states, February-June 2020. MMWR Morb Mortal Wkly Rep. 2020;69(33):1122-1126. doi:10.15585/mmwr.mm6933e1 - DOI - PMC - PubMed
-
- Ko JY, Danielson ML, Town M, et al. ; COVID-NET Surveillance Team . Risk factors for coronavirus disease 2019 (COVID-19)-associated hospitalization: COVID-19-Associated Hospitalization Surveillance Network and Behavioral Risk Factor Surveillance System. Clin Infect Dis. 2021;72(11):e695-e703. doi:10.1093/cid/ciaa1419 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
