

SARS-CoV-2 infection and venous thromboembolism after surgery: an international prospective cohort study
- PMID: 34428858
- PMCID: PMC8652887
- DOI: 10.1111/anae.15563
SARS-CoV-2 infection and venous thromboembolism after surgery: an international prospective cohort study
Abstract
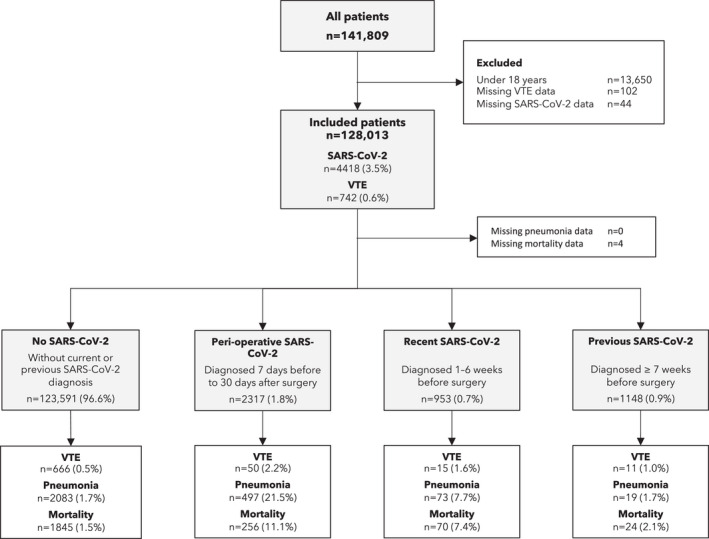
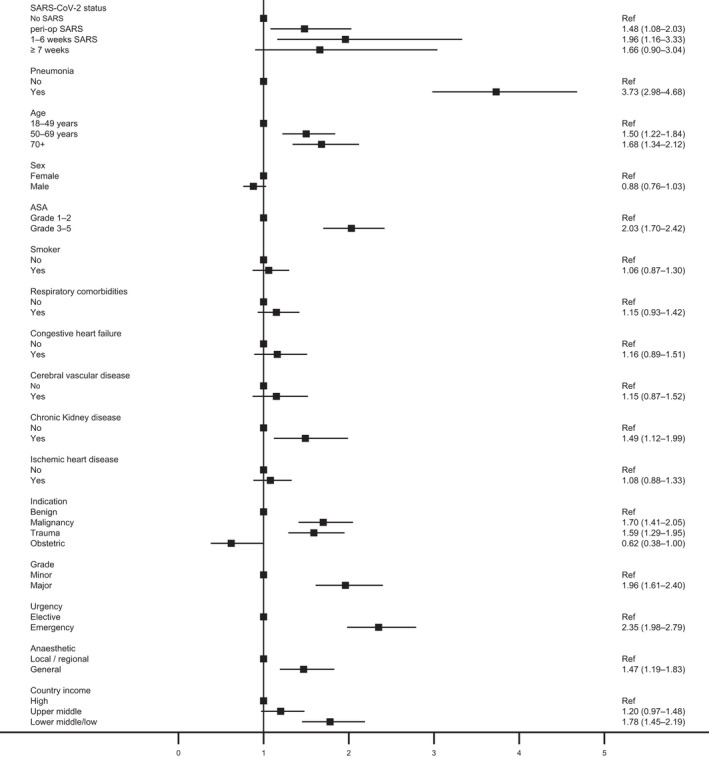
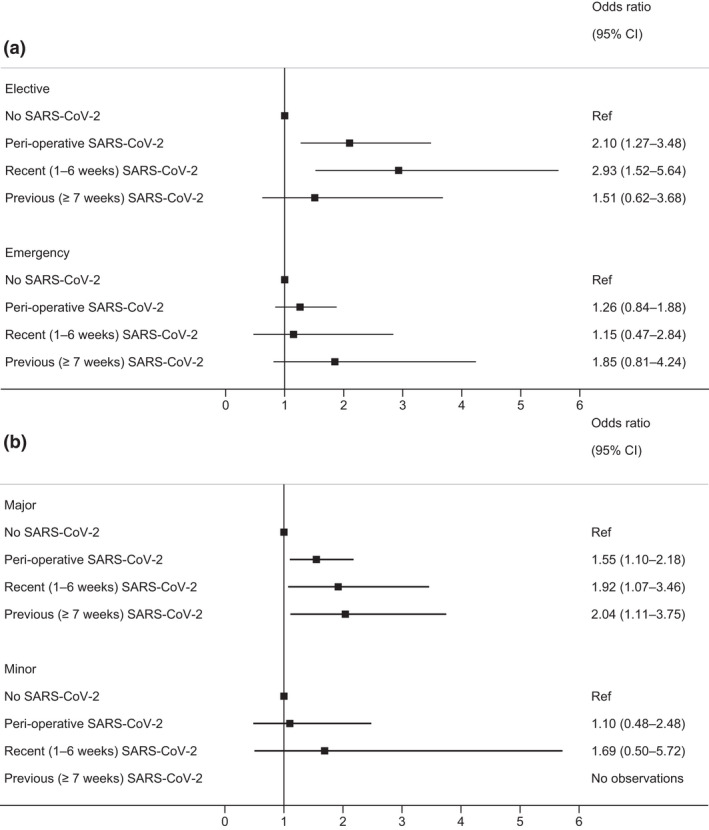
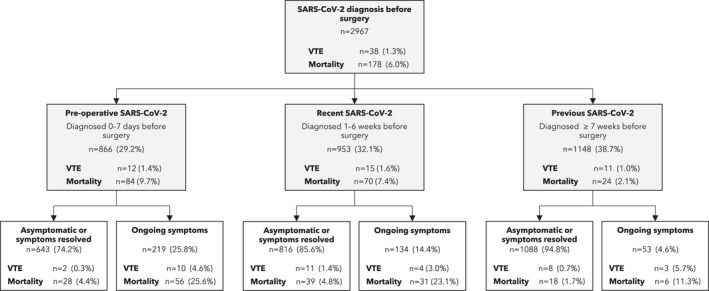
SARS-CoV-2 has been associated with an increased rate of venous thromboembolism in critically ill patients. Since surgical patients are already at higher risk of venous thromboembolism than general populations, this study aimed to determine if patients with peri-operative or prior SARS-CoV-2 were at further increased risk of venous thromboembolism. We conducted a planned sub-study and analysis from an international, multicentre, prospective cohort study of elective and emergency patients undergoing surgery during October 2020. Patients from all surgical specialties were included. The primary outcome measure was venous thromboembolism (pulmonary embolism or deep vein thrombosis) within 30 days of surgery. SARS-CoV-2 diagnosis was defined as peri-operative (7 days before to 30 days after surgery); recent (1-6 weeks before surgery); previous (≥7 weeks before surgery); or none. Information on prophylaxis regimens or pre-operative anti-coagulation for baseline comorbidities was not available. Postoperative venous thromboembolism rate was 0.5% (666/123,591) in patients without SARS-CoV-2; 2.2% (50/2317) in patients with peri-operative SARS-CoV-2; 1.6% (15/953) in patients with recent SARS-CoV-2; and 1.0% (11/1148) in patients with previous SARS-CoV-2. After adjustment for confounding factors, patients with peri-operative (adjusted odds ratio 1.5 (95%CI 1.1-2.0)) and recent SARS-CoV-2 (1.9 (95%CI 1.2-3.3)) remained at higher risk of venous thromboembolism, with a borderline finding in previous SARS-CoV-2 (1.7 (95%CI 0.9-3.0)). Overall, venous thromboembolism was independently associated with 30-day mortality (5.4 (95%CI 4.3-6.7)). In patients with SARS-CoV-2, mortality without venous thromboembolism was 7.4% (319/4342) and with venous thromboembolism was 40.8% (31/76). Patients undergoing surgery with peri-operative or recent SARS-CoV-2 appear to be at increased risk of postoperative venous thromboembolism compared with patients with no history of SARS-CoV-2 infection. Optimal venous thromboembolism prophylaxis and treatment are unknown in this cohort of patients, and these data should be interpreted accordingly.
Keywords: COVID-19; SARS-CoV-2; deep vein thrombosis; pulmonary embolism; venous thromboembolism.
© 2021 The Authors. Anaesthesia published by John Wiley & Sons Ltd on behalf of Association of Anaesthetists.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
