

Melanoma Cell Adhesion Molecule Expressing Helper T Cells in CNS Inflammatory Demyelinating Diseases
- PMID: 34429366
- PMCID: PMC8387012
- DOI: 10.1212/NXI.0000000000001069
Melanoma Cell Adhesion Molecule Expressing Helper T Cells in CNS Inflammatory Demyelinating Diseases
Abstract
Background and objective: To elucidate the relationship between melanoma cell adhesion molecule (MCAM)-expressing lymphocytes and pathogenesis of CNS inflammatory demyelinating diseases (IDDs).
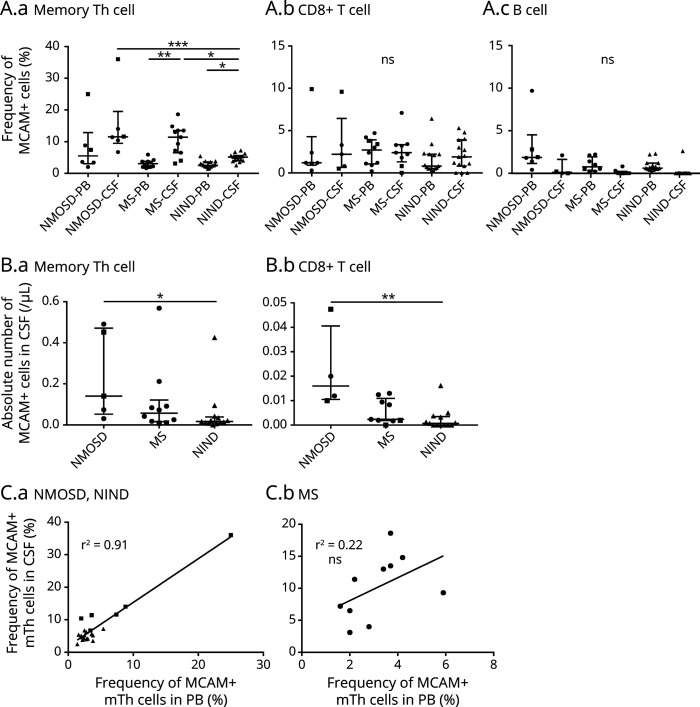
Methods: Patients with multiple sclerosis (MS) (n = 72) and neuromyelitis optica spectrum disorder (NMOSD, n = 29) were included. We analyzed the frequency and absolute numbers of MCAM+ lymphocytes (memory helper T [mTh] cells, naive helper T cells, CD8+ T cells, and B cells) in the peripheral blood (PB) and the CSF of patients with MS and NMOSD, treated with/without disease-modifying drugs (DMDs) or steroids, using flow cytometry.
Results: The frequency of MCAM+ cells was higher in the mTh cell subset than that in other lymphocyte subsets. A significant increase in the frequency and the absolute number of MCAM+ mTh cells was observed in the PB of patients with NMOSD, whereas no increase was observed in the PB of patients with MS. The frequency of CSF MCAM+ mTh cells was higher in relapsing patients with MS and NMOSD than that in the control group. Although there was no difference in the frequencies of MCAM+ lymphocytes among the DMD-treated groups, fingolimod decreased the absolute number of MCAM+ lymphocytes.
Discussion: MCAM+ mTh cells were elevated in the CSF of relapsing patients with MS and in both the PB and CSF of patients with NMOSD. These results indicate that MCAM contributes to the pathogenesis of MS and NMOSD through different mechanisms. MCAM could be a therapeutic target of CNS IDDs, and further study is needed to elucidate the underlying mechanism of MCAM in CNS IDD pathogenesis.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures


References
-
- McFarland HF, Martin R. Multiple sclerosis: a complicated picture of autoimmunity. Nat Immunol. 2007;8(9):913-919. - PubMed
-
- Dendrou CA, Fugger L, Friese MA. Immunopathology of multiple sclerosis. Nat Rev Immunol. 2015;15(9):545-558. - PubMed
-
- Panitch HS, Hirsch RL, Schindler J, Johnson KP. Treatment of multiple sclerosis with gamma interferon: exacerbations associated with activation of the immune system. Neurology. 1987;37(7):1097-1102. - PubMed
-
- Kebir H, Ifergan I, Alvarez JI, et al. Preferential recruitment of interferon-gamma-expressing TH17 cells in multiple sclerosis. Ann Neurol. 2009;66(3):390-402. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials