

Evaluation of a mechanical lung model to test small animal whole body plethysmography
- PMID: 34429449
- PMCID: PMC8384843
- DOI: 10.1038/s41598-021-96355-y
Evaluation of a mechanical lung model to test small animal whole body plethysmography
Abstract
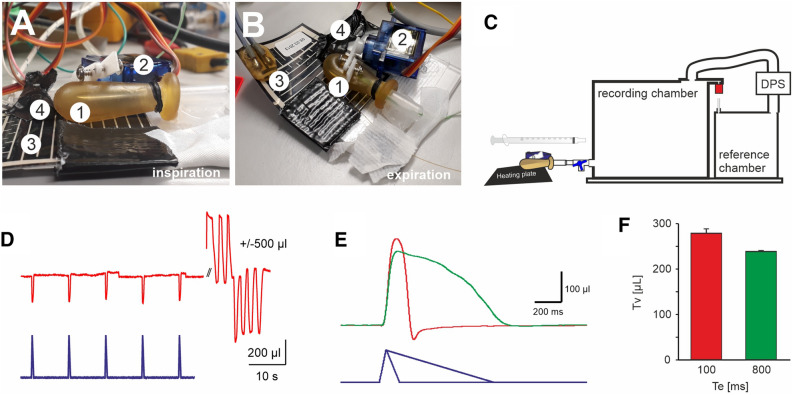
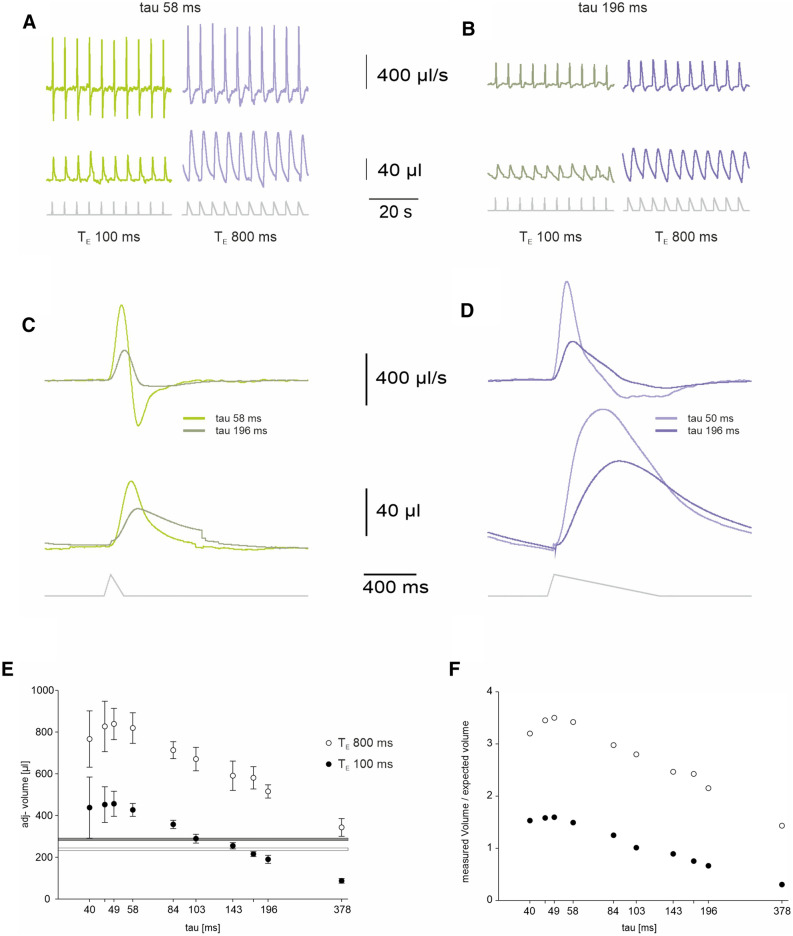
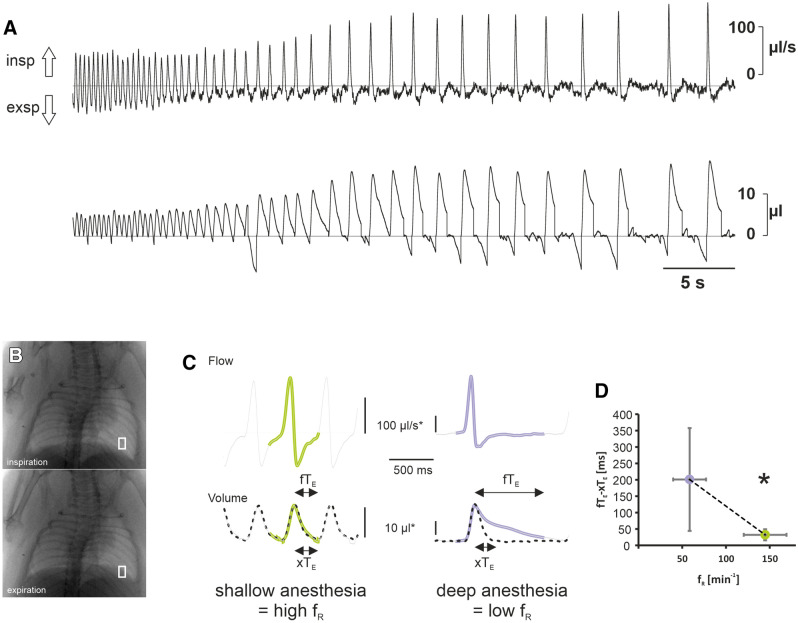
Whole-body plethysmography (WBP) is an established method to determine physiological parameters and pathophysiological alteration of breathing in animals and animal models of a variety of diseases. Although frequently used, there is ongoing debate about what exactly is measured by whole-body-plethysmography and how reliable the data derived from this method are. Here, we designed an artificial lung model that enables a thorough evaluation of different predictions about and around whole-body plethysmography. Using our lung model, we confirmed that during WBP two components contribute to the pressure changes detected in the chamber: (1) the increase in the pressure due to heating and moistening of the air during inspiration, termed conditioning; (2) changes in the chamber pressure that depend on airway resistance. Both components overlap and contribute to the temporal pressure-profile measured in the chamber or across the wall of the chamber, respectively. Our data showed that a precise measurement of the breathing volume appears to be hindered by at least two factors: (1) the unknown relative contribution of each of these two components; (2) not only the air in the inspired volume is conditioned during inspiration, but also air within the residual volume and dead space that is recruited during inspiration. Moreover, our data suggest that the expiratory negative pressure peak that is used to determine the enhanced pause (Penh) parameter is not a measure for airway resistance as such but rather a consequence of the animal's response to the airway resistance, using forced or active expiration to overcome the resistance by a higher thoracic pressure.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Vondráková K, Hoven RVD, Hirt RA. Adenosine 5'-monophosphate aerosol challenge does not provoke airflow limitation in healthy cats. Acta Vet. Brno. 2006;75:329–336. doi: 10.2754/avb200675030329. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
