

Identifying subtypes of bipolar disorder based on clinical and neurobiological characteristics
- PMID: 34429498
- PMCID: PMC8385023
- DOI: 10.1038/s41598-021-96645-5
Identifying subtypes of bipolar disorder based on clinical and neurobiological characteristics
Abstract
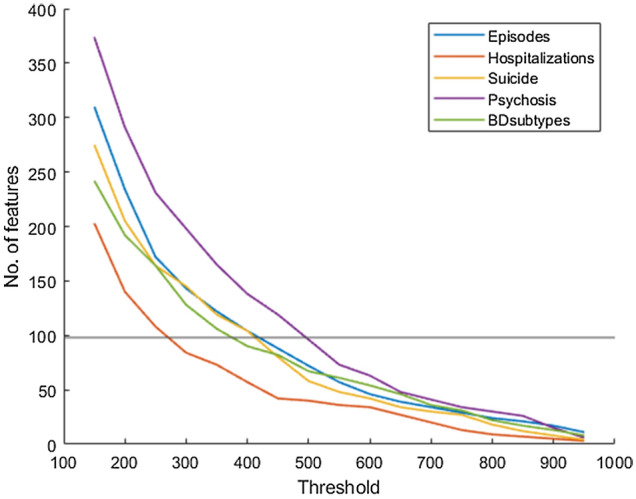
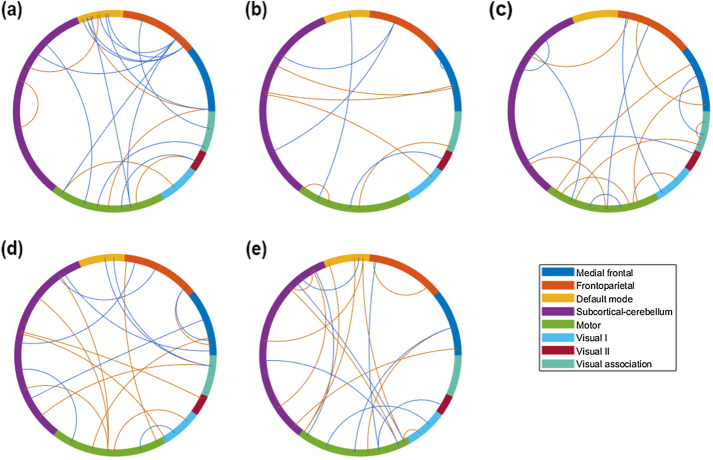
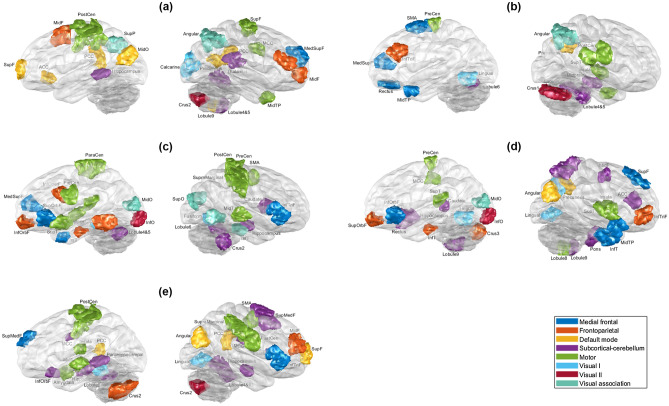
The ability to classify patients with bipolar disorder (BD) is restricted by their heterogeneity, which limits the understanding of their neuropathology. Therefore, we aimed to investigate clinically discernible and neurobiologically distinguishable BD subtypes. T1-weighted and resting-state functional magnetic resonance images of 112 patients with BD were obtained, and patients were segregated according to diagnostic subtype (i.e., types I and II) and clinical patterns, including the number of episodes and hospitalizations and history of suicide and psychosis. For each clinical pattern, fewer and more occurrences subgroups and types I and II were classified through nested cross-validation for robust performance, with minimum redundancy and maximum relevance, in feature selection. To assess the proportion of variance in cognitive performance explained by the neurobiological markers, multiple linear regression between verbal memory and the selected features was conducted. Satisfactory performance (mean accuracy, 73.60%) in classifying patients with a high or low number of episodes was attained through functional connectivity, mostly from default-mode and motor networks. Moreover, these neurobiological markers explained 62% of the variance in verbal memory. The number of episodes is a potentially critical aspect of the neuropathology of BD. Neurobiological markers can help identify BD neuroprogression.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Cognitive deficits in bipolar disorders: Implications for emotion.Clin Psychol Rev. 2018 Feb;59:126-136. doi: 10.1016/j.cpr.2017.11.006. Epub 2017 Nov 21. Clin Psychol Rev. 2018. PMID: 29195773 Free PMC article. Review.
-
Differential relations between fronto-limbic metabolism and executive function in patients with remitted bipolar I and bipolar II disorder.Bipolar Disord. 2012 Dec;14(8):831-42. doi: 10.1111/bdi.12017. Bipolar Disord. 2012. PMID: 23167933
-
Hippocampal volume and verbal memory performance in late-stage bipolar disorder.J Psychiatr Res. 2016 Feb;73:102-107. doi: 10.1016/j.jpsychires.2015.12.012. Epub 2015 Dec 15. J Psychiatr Res. 2016. PMID: 26714201 Free PMC article.
-
History of psychosis and previous episodes as potential explanatory factors for neurocognitive impairment in first-treatment bipolar I disorder.Bipolar Disord. 2016 Mar;18(2):136-47. doi: 10.1111/bdi.12377. Epub 2016 Mar 18. Bipolar Disord. 2016. PMID: 26990158
-
Neurobiological findings in bipolar II disorder compared with findings in bipolar I disorder.Can J Psychiatry. 2004 Dec;49(12):794-801. doi: 10.1177/070674370404901202. Can J Psychiatry. 2004. PMID: 15679202 Review.
Cited by
-
Atypical Functional Network Properties and Associated Dimensions of Child Psychopathology During Rest and Task Performance.Biol Psychiatry Glob Open Sci. 2022 Aug 7;3(3):541-549. doi: 10.1016/j.bpsgos.2022.07.007. eCollection 2023 Jul. Biol Psychiatry Glob Open Sci. 2022. PMID: 37519454 Free PMC article.
-
Classifying youth with bipolar disorder versus healthy youth using cerebral blood flow patterns.J Psychiatry Neurosci. 2023 Aug 29;48(4):E305-E314. doi: 10.1503/jpn.230012. Print 2023 Jul-Aug. J Psychiatry Neurosci. 2023. PMID: 37643801 Free PMC article.
-
Protocol for a systematic review and meta-analysis of coordinate-based network mapping of brain structure in bipolar disorder across the lifespan.BJPsych Open. 2023 Oct 9;9(6):e178. doi: 10.1192/bjo.2023.569. BJPsych Open. 2023. PMID: 37811544 Free PMC article.
-
Exploration of mood spectrum symptoms during a major depressive episode: The impact of contrapolarity-Results from a transdiagnostic cluster analysis on an Italian sample of unipolar and bipolar patients.Eur Psychiatry. 2022 May 31;65(1):e30. doi: 10.1192/j.eurpsy.2022.20. Eur Psychiatry. 2022. PMID: 35638732 Free PMC article.
