

Clinical correlates of circulating cell-free DNA tumor fraction
- PMID: 34432811
- PMCID: PMC8386888
- DOI: 10.1371/journal.pone.0256436
Clinical correlates of circulating cell-free DNA tumor fraction
Abstract
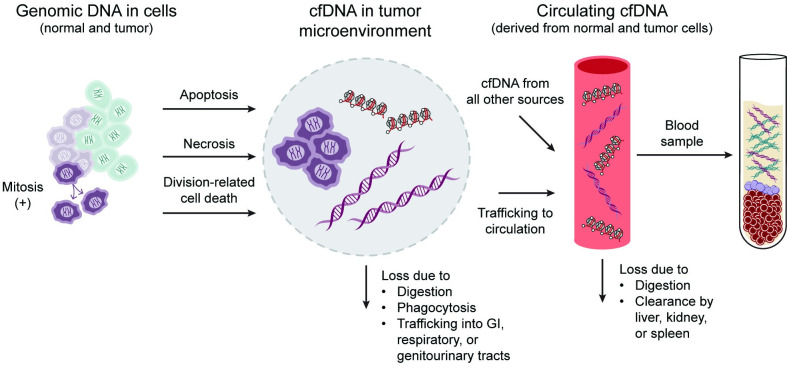
Background: Oncology applications of cell-free DNA analysis are often limited by the amount of circulating tumor DNA and the fraction of cell-free DNA derived from tumor cells in a blood sample. This circulating tumor fraction varies widely between individuals and cancer types. Clinical factors that influence tumor fraction have not been completely elucidated.
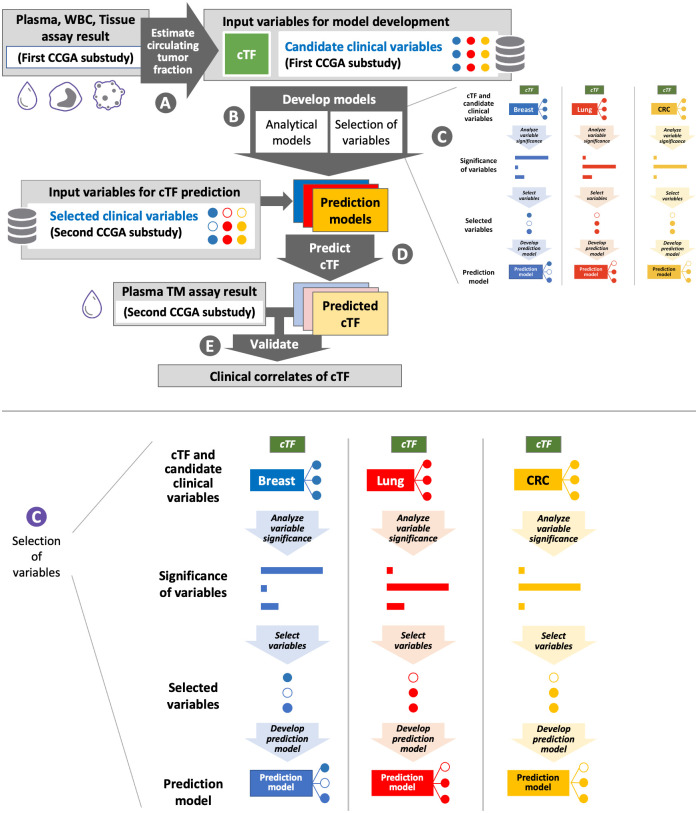
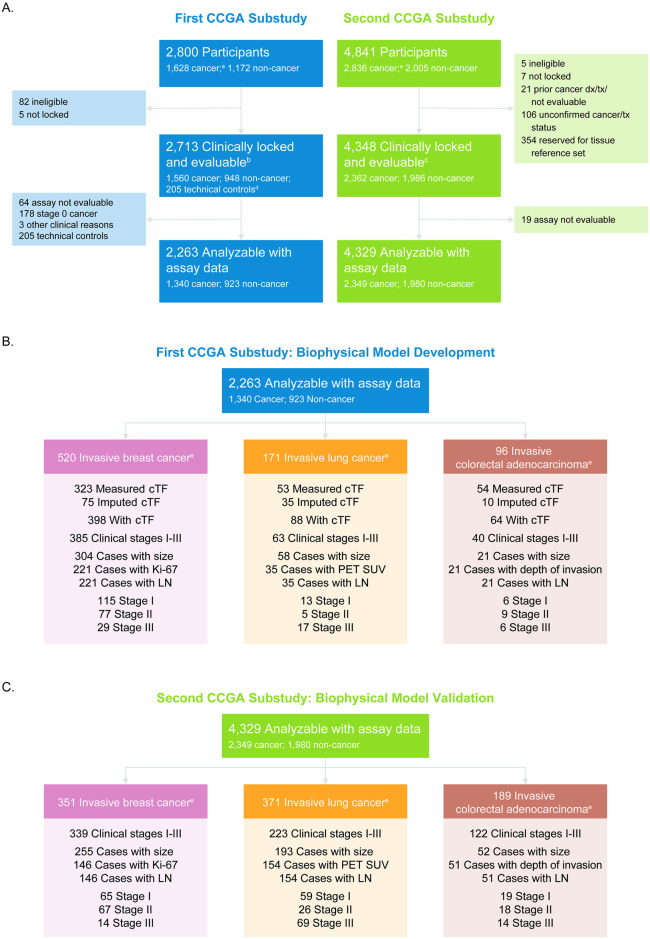
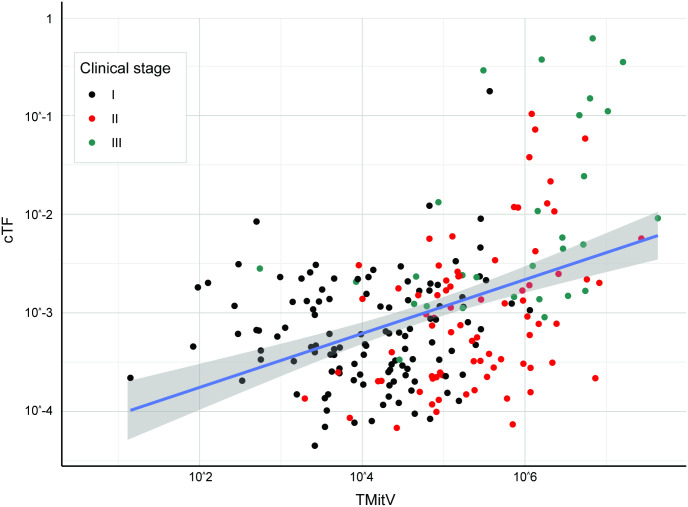
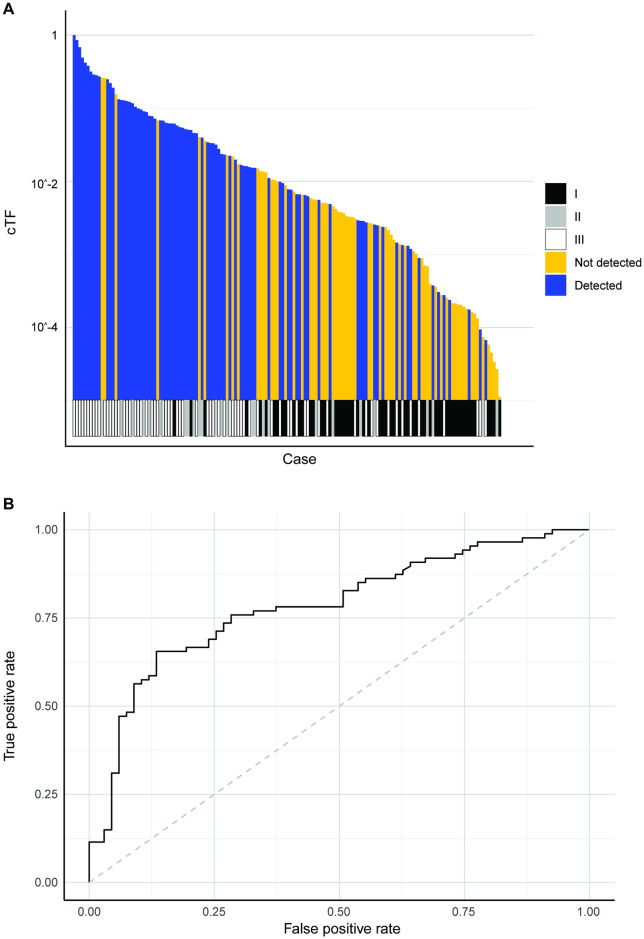
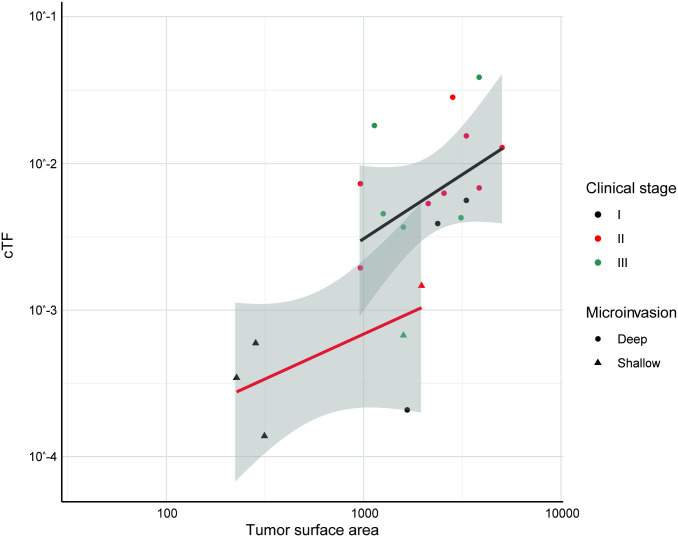
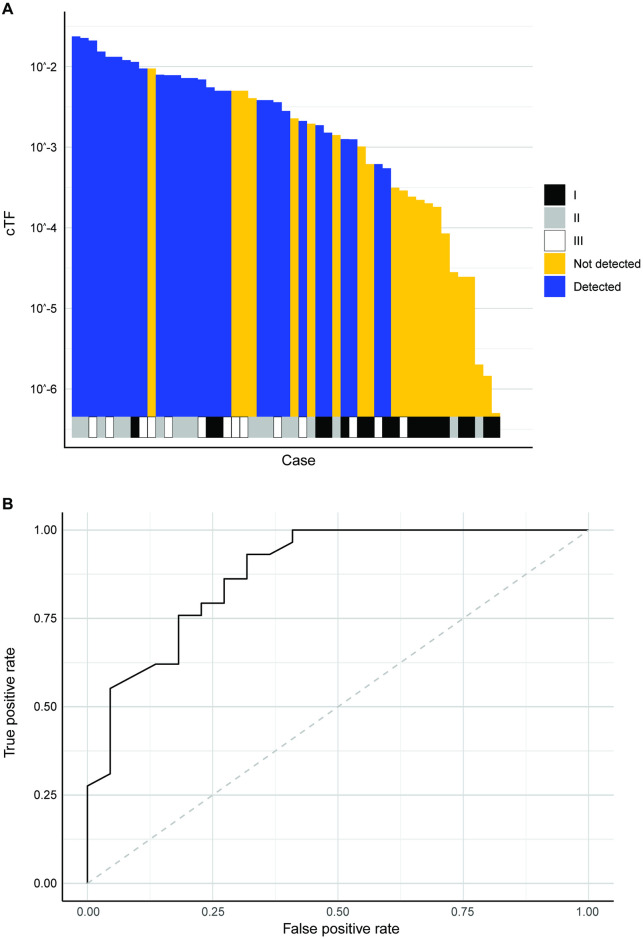
Methods and findings: Circulating tumor fraction was determined for breast, lung, and colorectal cancer participant samples in the first substudy of the Circulating Cell-free Genome Atlas study (CCGA; NCT02889978; multi-cancer early detection test development) and was related to tumor and patient characteristics. Linear models were created to determine the influence of tumor size combined with mitotic or metabolic activity (as tumor mitotic volume or excessive lesion glycolysis, respectively), histologic type, histologic grade, and lymph node status on tumor fraction. For breast and lung cancer, tumor mitotic volume and excessive lesion glycolysis (primary lesion volume scaled by percentage positive for Ki-67 or PET standardized uptake value minus 1.0, respectively) were the only statistically significant covariates. For colorectal cancer, the surface area of tumors invading beyond the subserosa was the only significant covariate. The models were validated with cases from the second CCGA substudy and show that these clinical correlates of circulating tumor fraction can predict and explain the performance of a multi-cancer early detection test.
Conclusions: Prognostic clinical variables, including mitotic or metabolic activity and depth of invasion, were identified as correlates of circulating tumor DNA by linear models that relate clinical covariates to tumor fraction. The identified correlates indicate that faster growing tumors have higher tumor fractions. Early cancer detection from assays that analyze cell-free DNA is determined by circulating tumor fraction. Results support that early detection is particularly sensitive for faster growing, aggressive tumors with high mortality, many of which have no available screening today.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: Author J.B. is an employee of GRAIL, Inc. with equity in the company, and holds equity in Roche. Author J.L. was an employee of GRAIL, Inc. at the time of the study, and is currently an employee of Genentech, Inc. (South San Francisco, CA). Authors O.V. and A.J. are employees of GRAIL, Inc. with equity in the company, and hold equity in Illumina. Author A.M.A. was an employee of GRAIL, Inc. at the time of the study, is currently an employee of Illumina, Inc. (San Diego, CA), and is an advisor to and an equity holder in Foresite Labs and Myst Therapeutics. Since submission of this article for peer review at PLOS ONE, GRAIL, Inc. has launched a commercially available multi-cancer early detection test product (GalleriTM). We confirmed that this does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures





References
-
- Corcoran RB. Circulating Tumor DNA: Clinical Monitoring and Early Detection. Annu Rev Cancer Biol. 2019;3: 187–201. doi: 10.1146/annurev-cancerbio-030518-055719 - DOI
-
- Venn O, Hubbell E, Sakarya O, Chang C, Halks-Miller M, Steffen K, et al. Tumor shedding into cell-free DNA (cfDNA) is associated with high-mortality cancers [poster]. 31st Annual Meeting on The Biology of Genomes. Cold Spring Harbor, NY: Cold Spring Harbor Laboratory; 2019. https://meetings.cshl.edu/abstracts.aspx?meet=GENOME&year=19
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
