

Postoperative analgesic effects of paravertebral block versus erector spinae plane block for thoracic and breast surgery: A meta-analysis
- PMID: 34432822
- PMCID: PMC8386864
- DOI: 10.1371/journal.pone.0256611
Postoperative analgesic effects of paravertebral block versus erector spinae plane block for thoracic and breast surgery: A meta-analysis
Abstract
Background: Paravertebral block (PVB) is the most recognized regional anesthesia technique after thoracic epidural anesthesia for postoperative analgesia in thoracic and breast surgery. Erector spinae plane block (ESPB) is a recently discovered blocking technique, and it has evidenced excellent postoperative analgesia for breast and thoracic surgery with fewer adverse reactions. However, there are controversies about the postoperative analgesic effects of the two analgesic techniques.
Objective: To assess the analgesic effects of PVB versus ESPB in postoperative thoracic and breast surgery.
Methods: We systematically searched PubMed, Cochrane Library, EMBASE, Web of Science, and ScienceDirect databases up to April 5, 2021. The primary outcome was postoperative pain scores. Secondary outcomes included: opioid consumption, additional analgesia, postoperative nausea and vomiting (PONV) 24 hours post-operation, and the time required for completing block procedure. This study was registered in PROSPERO, number CRD42021246160.
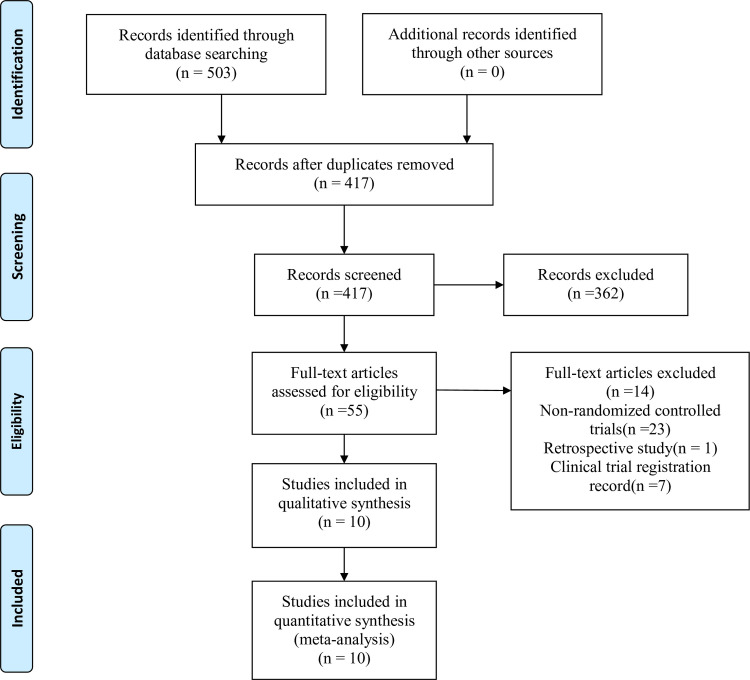
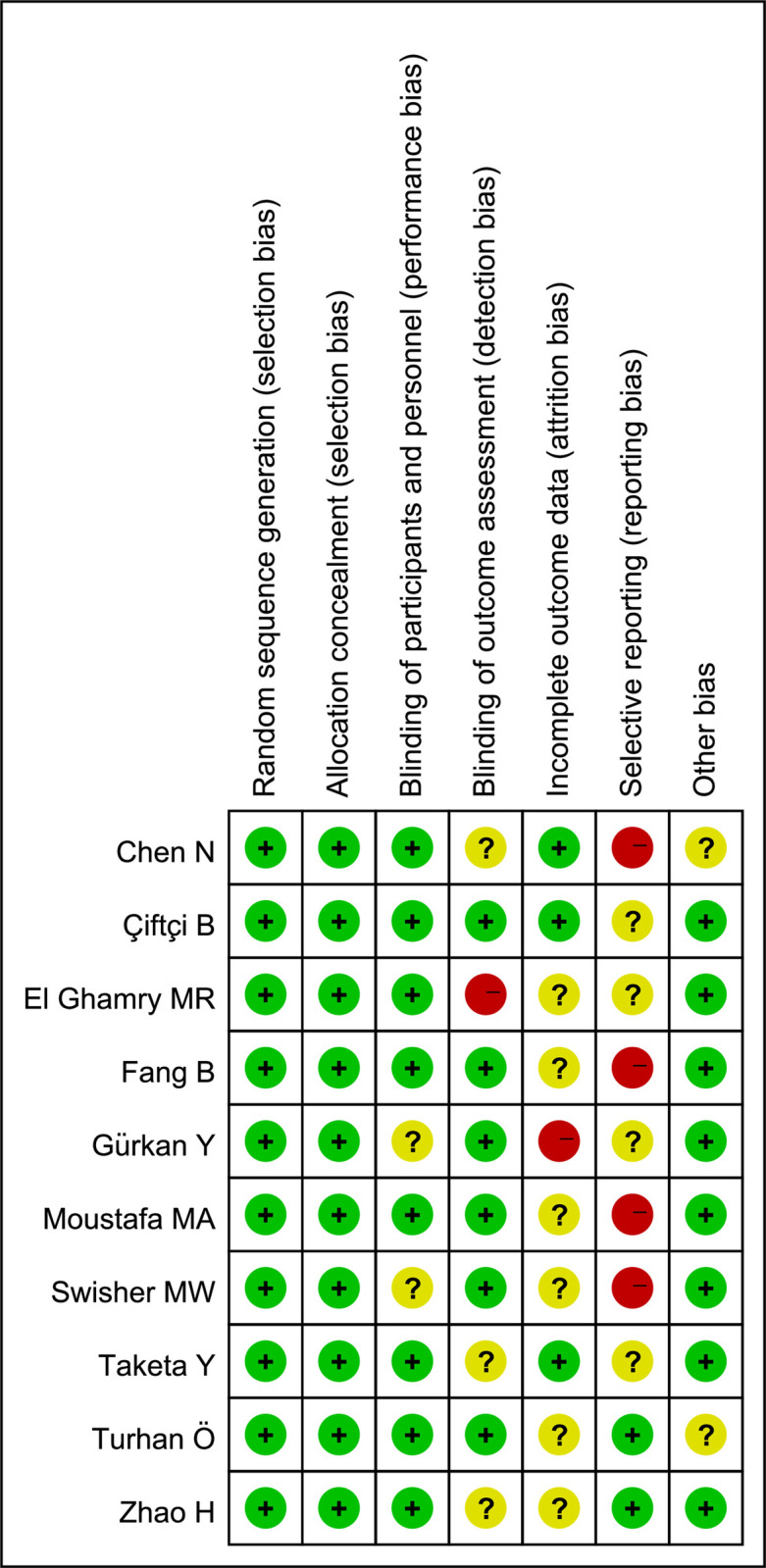
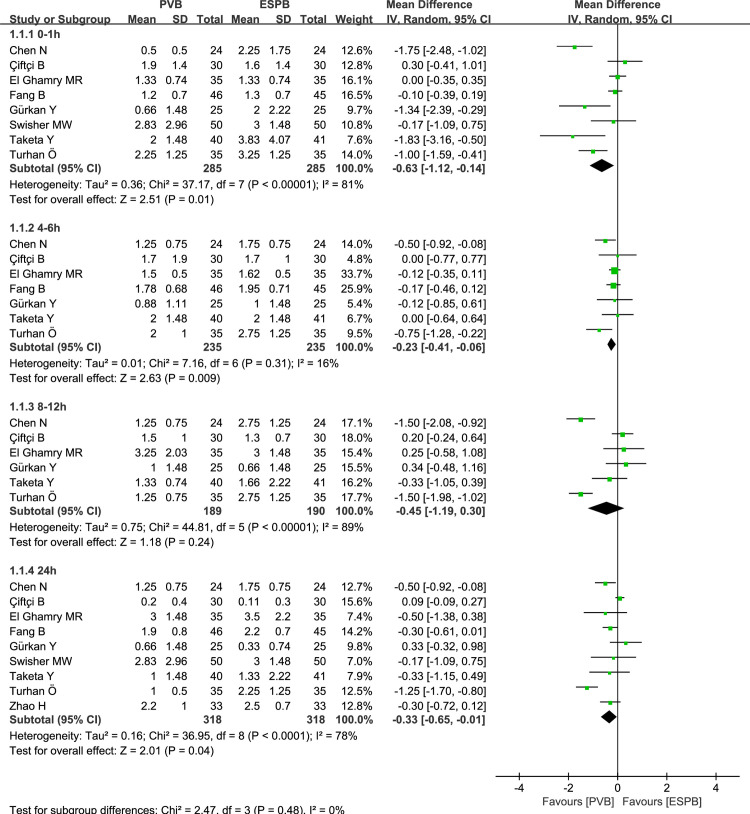
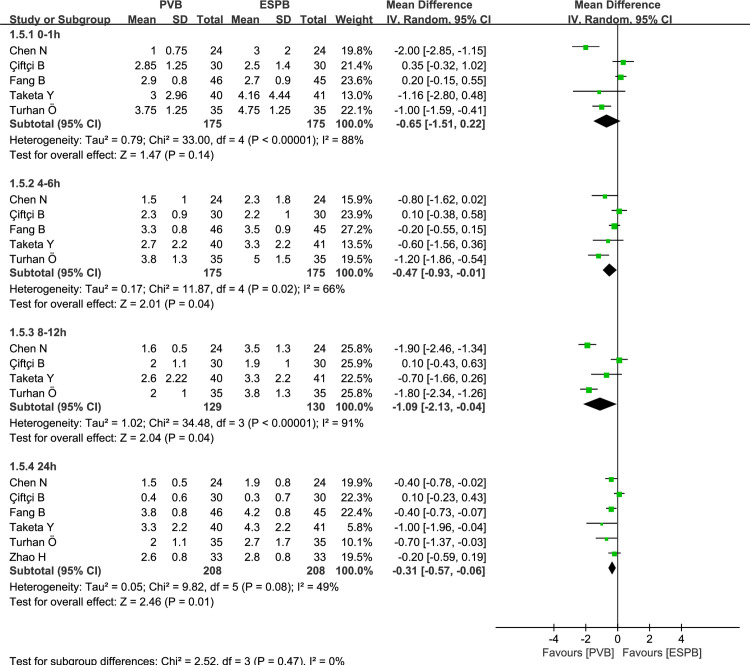
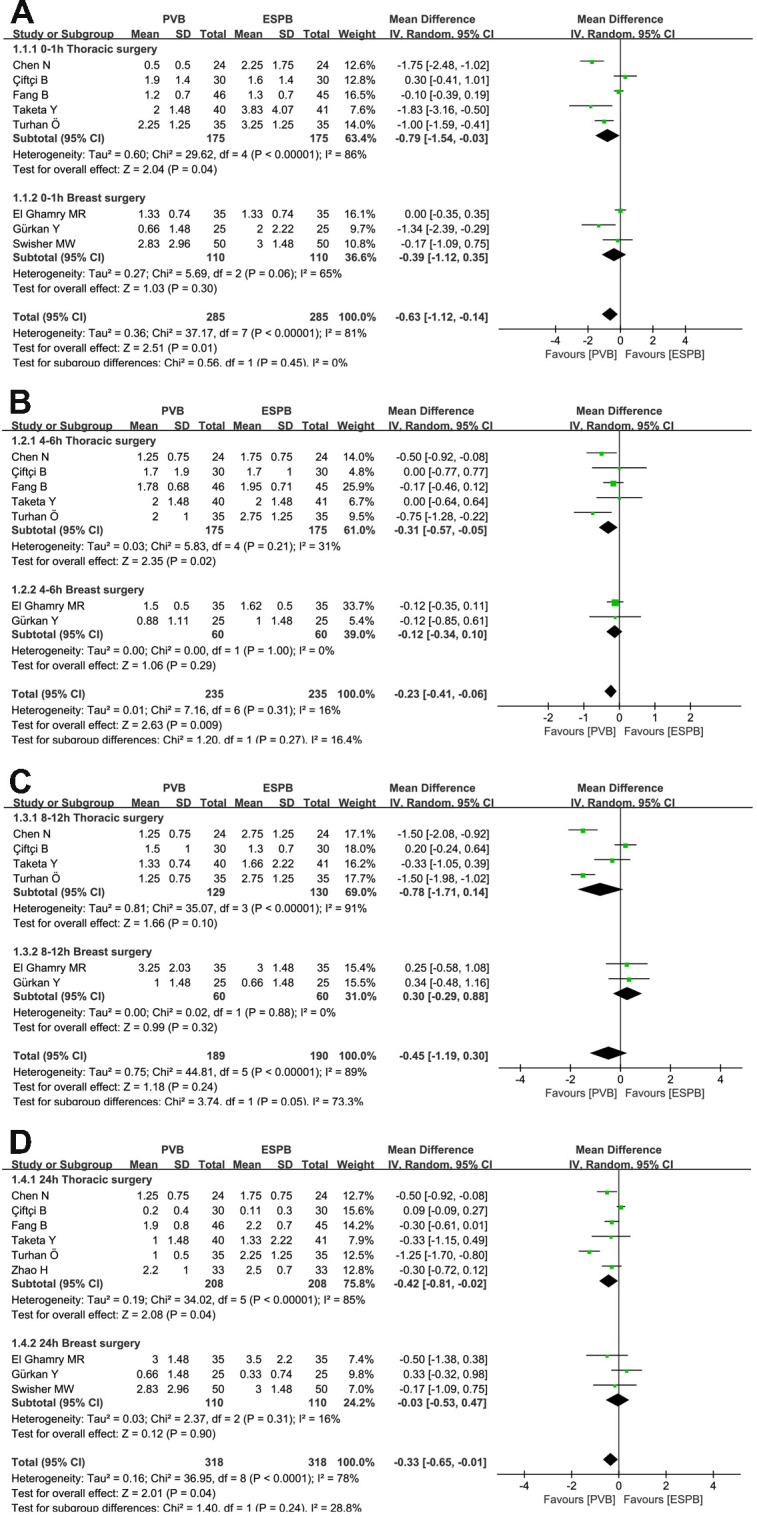
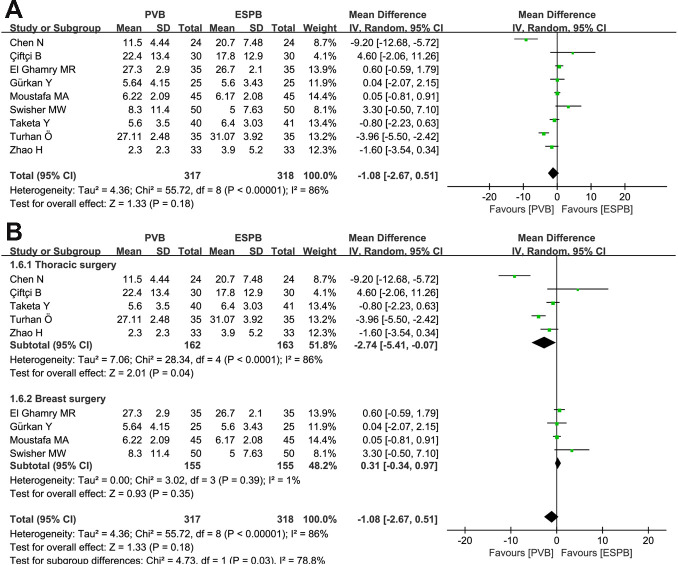
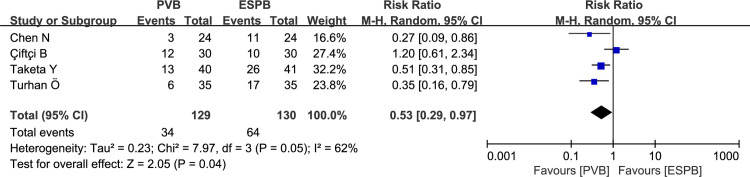
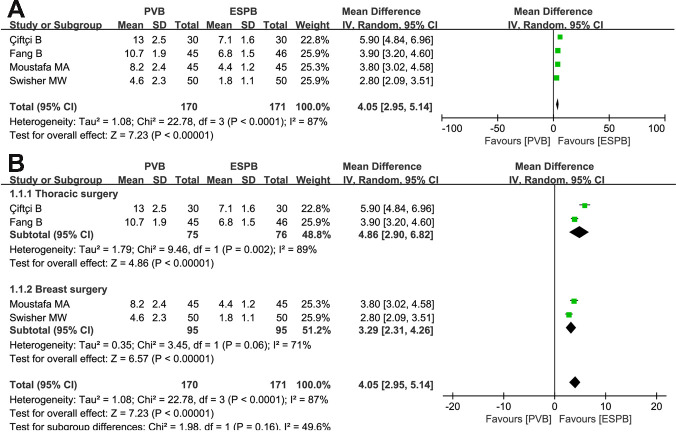
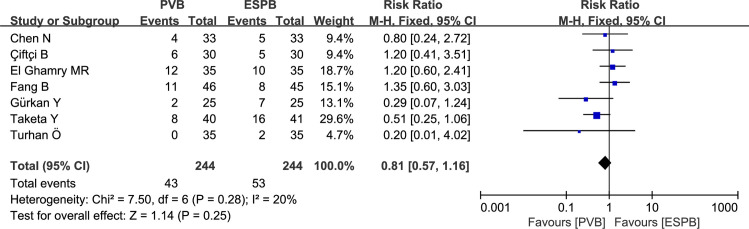
Results: After screening relevant, full-text articles, ten randomized controlled trials (RCTs) that met the inclusion criteria were retrieved for this meta-analysis. Six studies involved thoracic surgery patients, and four included breast surgery patients. Thoracic surgery studies included all of the outcomes involved in this meta-analysis while breast surgery did not report pain scores at movement and additional analgesia in 24 hours post-operation. For thoracic surgery, PVB resulted in significant reduction in the following pain scores: 0-1 hours (MD = -0.79, 95% CI: -1.54 to -0.03, P = 0.04), 4-6 hours (MD = -0.31, 95% CI: -0.57 to -0.05, P = 0.02), and 24 hours (MD = -0.42, 95% CI: -0.81 to -0.02, P = 0.04) at rest; significant reduction in pain scores at 4-6 hours (MD = -0.47, 95% CI: -0.93 to -0.01, P = 0.04), 8-12 hours (MD = -1.09, 95% CI: -2.13 to -0.04, P = 0.04), and 24 hours (MD = -0.31, 95% CI: -0.57 to -0.06, P = 0.01) at movement. Moreover, the opioid consumption at 24 hours post-operation (MD = -2.74, 95% CI: -5.41 to -0.07, P = 0.04) and the incidence of additional analgesia in 24 hours of the postoperative course (RR: 0.53, 95% CI: 0.29 to 0.97, P = 0.04) were significantly lower in the PVB group than in the ESPB group for thoracic surgery. However, no significant differences were found in pain scores at rest at various time points postoperatively, and opioid consumption at 24 hours post-operation for breast surgery. The time required for completing block procedure was longer in the PVB group than in the ESPB group for thoracic and breast surgery, and the incidence of PONV between the two groups showed no significant difference.
Conclusion: The postoperative analgesic effects of PVB versus ESPB are distinguished by the surgical site. For thoracic surgery, the postoperative analgesic effect of PVB is better than that of ESPB. For breast surgery, the postoperative analgesic effects of PVB and ESPB are similar.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
