

Coronavirus Disease 2019 (COVID-19) Pandemic and Pregnancy Outcomes in a U.S. Population
- PMID: 34433180
- PMCID: PMC8454282
- DOI: 10.1097/AOG.0000000000004547
Coronavirus Disease 2019 (COVID-19) Pandemic and Pregnancy Outcomes in a U.S. Population
Abstract
Objective: To examine whether the coronavirus disease 2019 (COVID-19) pandemic altered risk of adverse pregnancy-related outcomes and whether there were differences by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection status among pregnant women.
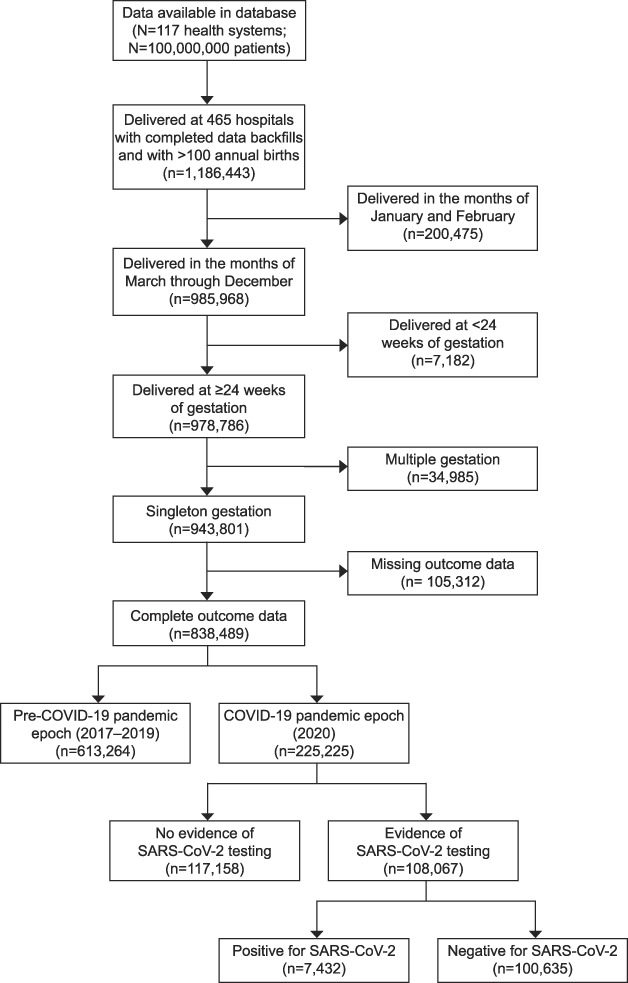
Methods: In this retrospective cohort study using Epic's Cosmos research platform, women who delivered during the pandemic (March-December 2020) were compared with those who delivered prepandemic (matched months 2017-2019). Within the pandemic epoch, those who tested positive for SARS-CoV-2 infection were compared with those with negative test results or no SARS-CoV-2 diagnosis. Comparisons were performed using standardized differences, with a value greater than 0.1 indicating meaningful differences between groups.
Results: Among 838,489 women (225,225 who delivered during the pandemic), baseline characteristics were similar between epochs. There were no significant differences in adverse pregnancy outcomes between epochs (standardized difference<0.10). In the pandemic epoch, 108,067 (48.0%) women had SARS-CoV-2 testing available; of those, 7,432 (6.9%) had positive test results. Compared with women classified as negative for SARS-CoV-2 infection, those who tested positive for SARS-CoV-2 infection were less likely to be non-Hispanic White or Asian or to reside in the Midwest and more likely to be Hispanic, have public insurance, be obese, and reside in the South or in high social vulnerability ZIP codes. There were no significant differences in the frequency of preterm birth (8.5% vs 7.6%, standardized difference=0.032), stillbirth (0.4% vs 0.4%, standardized difference=-0.002), small for gestational age (6.4% vs 6.5%, standardized difference=-0.002), large for gestational age (7.7% vs 7.7%, standardized difference=-0.001), hypertensive disorders of pregnancy (16.3% vs 15.8%, standardized difference=0.014), placental abruption (0.5% vs 0.4%, standardized difference=0.007), cesarean birth (31.2% vs 29.4%, standardized difference=0.039), or postpartum hemorrhage (3.4% vs 3.1%, standardized difference=0.019) between those who tested positive for SARS-CoV-2 infection and those classified as testing negative.
Conclusion: In a geographically diverse U.S. cohort, the frequency of adverse pregnancy-related outcomes did not differ between those delivering before compared with during the pandemic, nor between those classified as positive compared with negative for SARS-CoV-2 infection during pregnancy.
Copyright © 2021 by the American College of Obstetricians and Gynecologists. Published by Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Financial Disclosure Eric Lindgren, Kieran Gallagher, and Justin Y. Lo disclosed that they are employees of Epic Systems Corporation, a health IT software company that provides Cosmos, a research platform containing data from Epic's health care provider customer organizations. Epic licenses electronic health record software and provides related services to health care organizations that pay Epic for such software and services. The authors and Epic and have no conflicts of interest with respect to the subject matter of this study but would like to clarify that insights gleaned from this research may inform Epic's software design and development activities. Heather H. Burris disclosed that money was paid to her institution from Highmark Blue Cross Blue Shield Delaware's donor-advised fund (foundation grant), BluePrints for the Community, and Independence Blue Cross. The other authors did not report any potential conflicts of interest.
Figures
Comment in
-
Coronavirus Disease 2019 (COVID-19) and Pregnancy Outcomes: State of the Science.Obstet Gynecol. 2021 Oct 1;138(4):539-541. doi: 10.1097/AOG.0000000000004548. Obstet Gynecol. 2021. PMID: 34433179 Free PMC article. No abstract available.
References
-
- Centers for Disease Control and Prevention COVID Data Tracker. Accessed July 5, 2021. https://covid.cdc.gov/covid-data-tracker/#datatracker-home
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
