

Neurofilament light and heterogeneity of disease progression in amyotrophic lateral sclerosis: development and validation of a prediction model to improve interventional trials
- PMID: 34433481
- PMCID: PMC8390195
- DOI: 10.1186/s40035-021-00257-y
Neurofilament light and heterogeneity of disease progression in amyotrophic lateral sclerosis: development and validation of a prediction model to improve interventional trials
Abstract
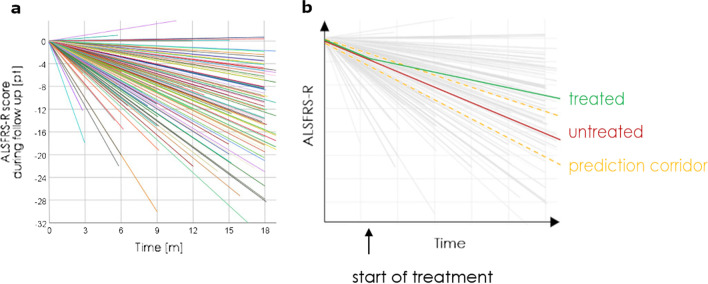
Background: Interventional trials in amyotrophic lateral sclerosis (ALS) suffer from the heterogeneity of the disease as it considerably reduces statistical power. We asked if blood neurofilament light chains (NfL) could be used to anticipate disease progression and increase trial power.
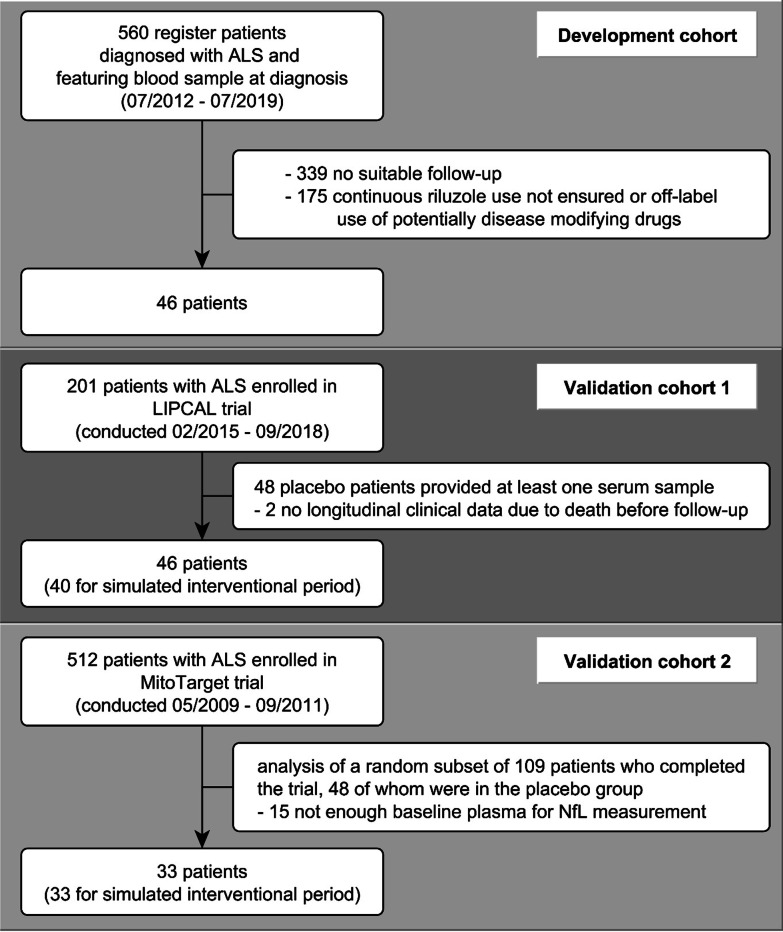
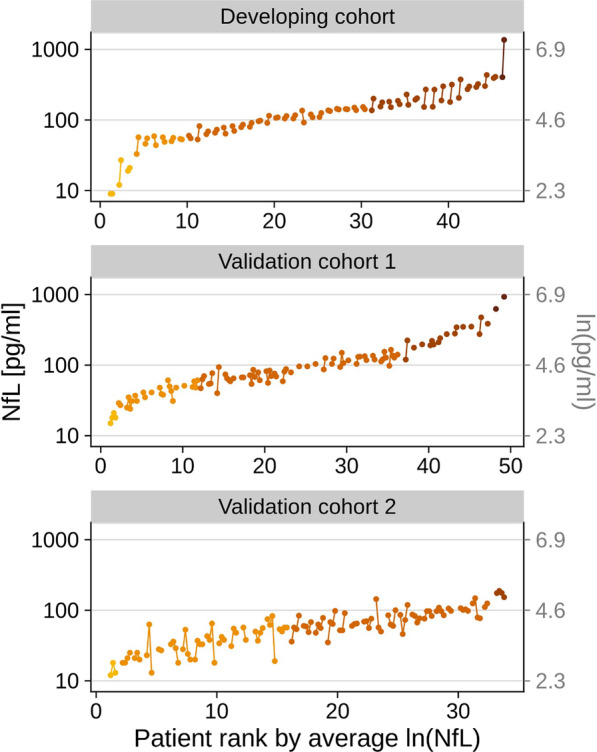
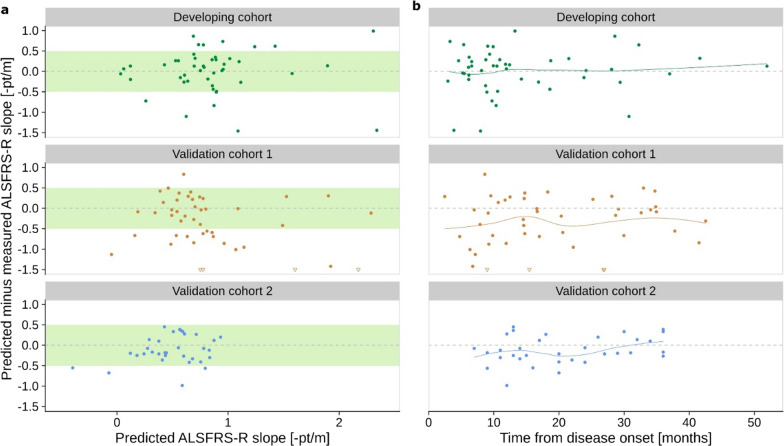
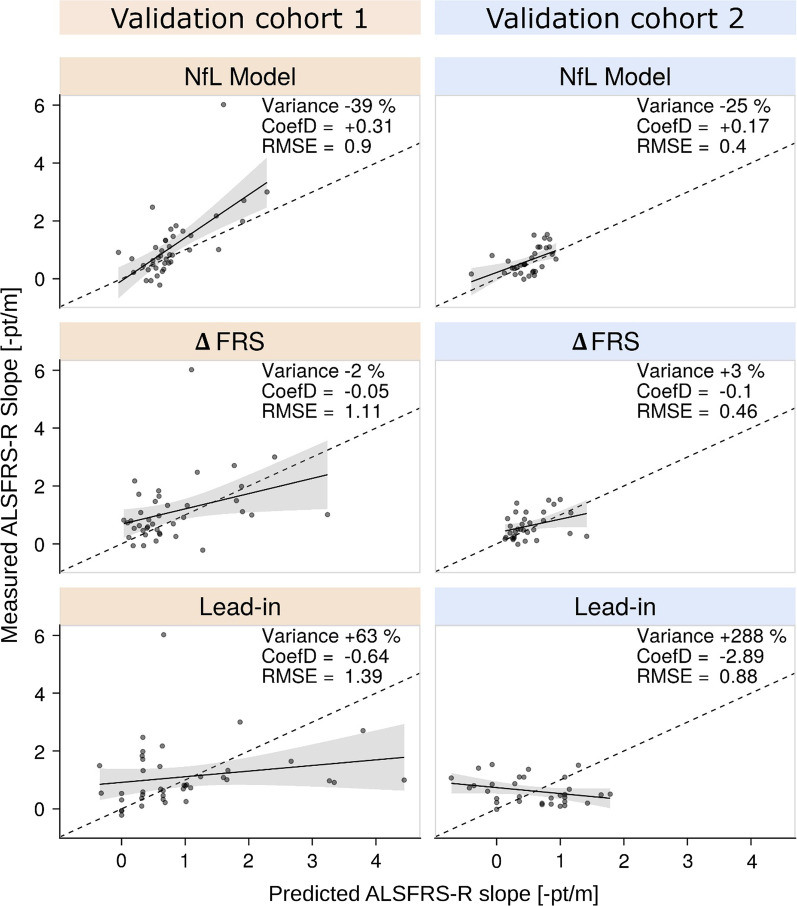
Methods: In 125 patients with ALS from three independent prospective studies-one observational study and two interventional trials-we developed and externally validated a multivariate linear model for predicting disease progression, measured by the monthly decrease of the ALS Functional Rating Scale Revised (ALSFRS-R) score. We trained the prediction model in the observational study and tested the predictive value of the following parameters assessed at diagnosis: NfL levels, sex, age, site of onset, body mass index, disease duration, ALSFRS-R score, and monthly ALSFRS-R score decrease since disease onset. We then applied the resulting model in the other two study cohorts to assess the actual utility for interventional trials. We analyzed the impact on trial power in mixed-effects models and compared the performance of the NfL model with two currently used predictive approaches, which anticipate disease progression using the ALSFRS-R decrease during a three-month observational period (lead-in) or since disease onset (ΔFRS).
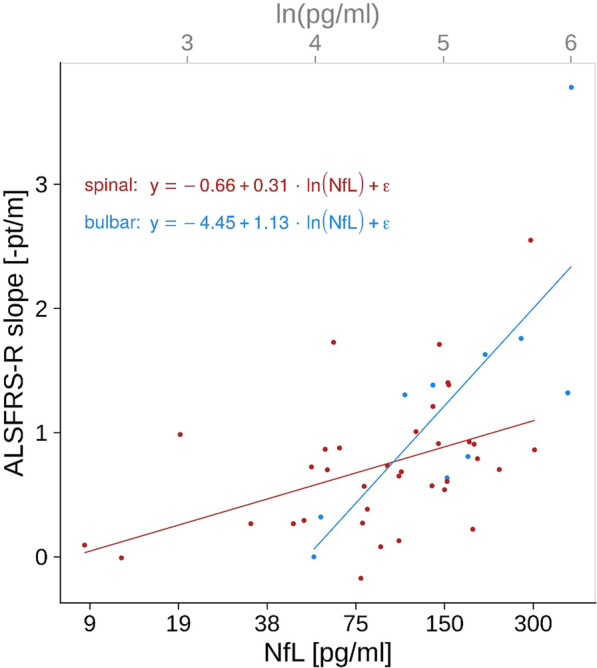
Results: Among the parameters provided, the NfL levels (P < 0.001) and the interaction with site of onset (P < 0.01) contributed significantly to the prediction, forming a robust NfL prediction model (R = 0.67). Model application in the trial cohorts confirmed its applicability and revealed superiority over lead-in and ΔFRS-based approaches. The NfL model improved statistical power by 61% and 22% (95% confidence intervals: 54%-66%, 7%-29%).
Conclusion: The use of the NfL-based prediction model to compensate for clinical heterogeneity in ALS could significantly increase the trial power. NCT00868166, registered March 23, 2009; NCT02306590, registered December 2, 2014.
Keywords: Amyotrophic lateral sclerosis; Disease progression; Interventional trials; Neurofilament light; Prediction model; Statistical power.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
