

Reversible Leukoencephalopathy in a Man with Childhood-onset Hyperornithinemia-Hyperammonemia-Homocitrullinuria Syndrome
- PMID: 34433721
- PMCID: PMC8907781
- DOI: 10.2169/internalmedicine.7843-21
Reversible Leukoencephalopathy in a Man with Childhood-onset Hyperornithinemia-Hyperammonemia-Homocitrullinuria Syndrome
Abstract
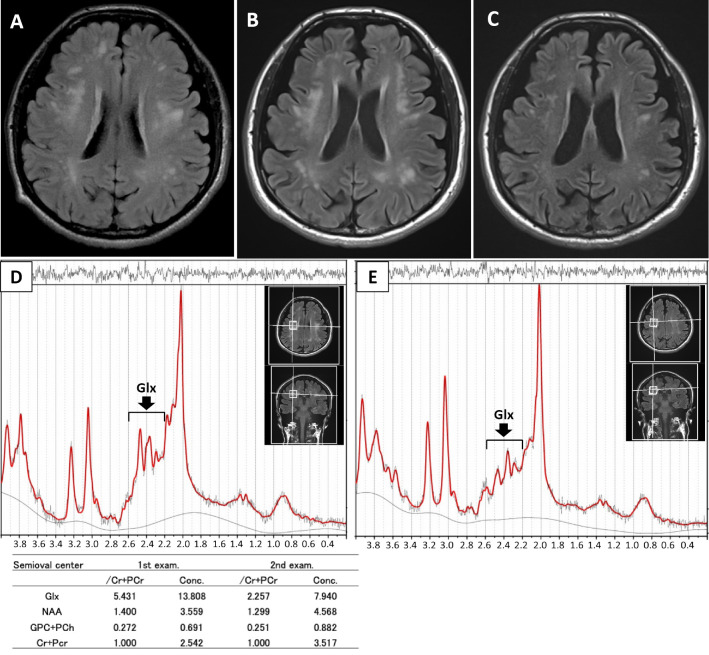
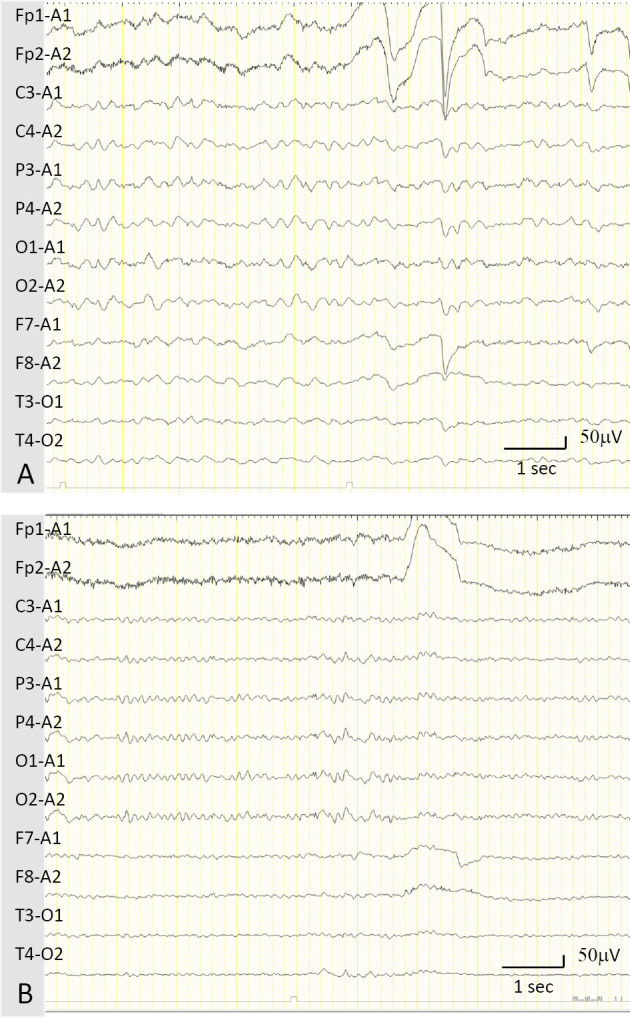
A 49-year-old Japanese man had shown developmental delay, learning difficulties, epilepsy, and slowly progressive gait disturbance in elementary school. At 46 years old, he experienced repeated drowsiness with or without generalized convulsions, and hyperammonemia was detected. Brain magnetic resonance imaging detected multiple cerebral white matter lesions. An electroencephalogram showed diffuse slow basic activities with 2- to 3-Hz δ waves. Genetic tests confirmed a diagnosis of hyperornithinemia-hyperammonemia-homocitrullinuria (HHH) syndrome. Leukoencephalopathy was resolved following the administration of L-arginine and lactulose with a decrease in plasma ammonia levels and glutamine-glutamate peak on magnetic resonance spectroscopy. Leukoencephalopathy in HHH syndrome may be reversible with the resolution of hyperammonemia-induced glutamine toxicity.
Keywords: HHH syndrome; MRS; glutamine toxicity; hyperammonemia; leukoencephalopathy; magnetic resonance spectroscopy.
Conflict of interest statement
Figures
References
-
- Camacho J, Rioseco-Camacho N. Hyperornithinemia-hyperammonemia-homocitrullinuria syndrome. In: GeneReviews™ [Internet]. Pagon RA, Bird TD, Dolan CR, Stephens K, Adam MP, Eds. University of Washington, Seattle, 2012: 1993-2021. - PubMed
-
- Camacho JA, Obie C, Biery B, et al. . Hyperornithinaemia-hyperammonaemia-homocitrullinuria syndrome is caused by mutations in a gene encoding a mitochondrial ornithine transporter. Nat Genet 22: 151-158, 1999. - PubMed
-
- Oyanagi K, Tsuchiyama A, Itakura Y, et al. . The mechanism of hyperammonaemia and hyperornithinaemia in the syndrome of hyperornithinaemia, hyperammonaemia with homocitrullinuria. J Inherit Metab Dis 6: 133-134, 1983. - PubMed
-
- Koike R, Fujimori K, Yuasa T, Miyatake T, Inoue I, Saheki T. Hyperornithinemia, hyperammonemia, and homocitrullinuria: case report and biochemical study. Neurology 37: 1813-1815, 1987. - PubMed