

Current Concepts on Subtalar Instability
- PMID: 34435065
- PMCID: PMC8381447
- DOI: 10.1177/23259671211021352
Current Concepts on Subtalar Instability
Abstract
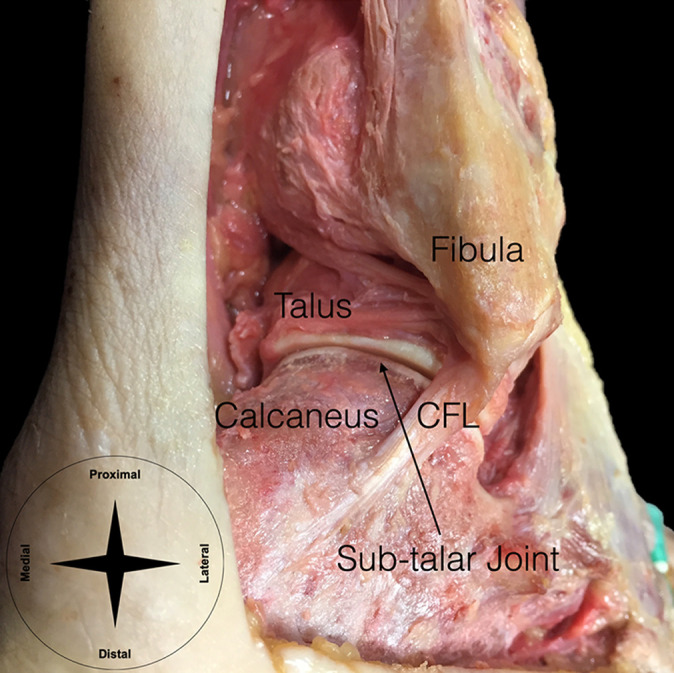
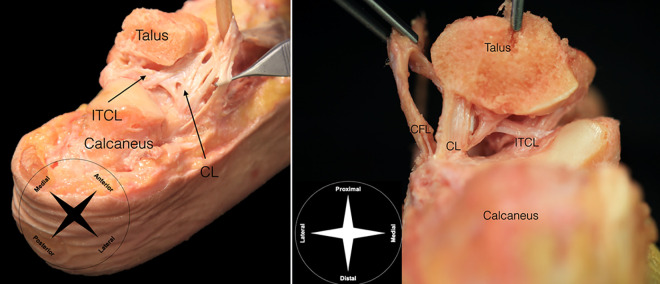
Subtalar instability remains a topic of debate, and its precise cause is still unknown. The mechanism of injury and clinical symptoms of ankle and subtalar instabilities largely overlap, resulting in many cases of isolated or combined subtalar instability that are often misdiagnosed. Neglecting the subtalar instability may lead to failure of conservative or surgical treatment and result in chronic ankle instability. Understanding the accurate anatomy and biomechanics of the subtalar joint, their interplay, and the contributions of the different subtalar soft tissue structures is fundamental to correctly diagnose and manage subtalar instability. An accurate diagnosis is crucial to correctly identify those patients with instability who may require conservative or surgical treatment. Many different nonsurgical and surgical approaches have been proposed to manage combined or isolated subtalar instability, and the clinician should be aware of available treatment options to make an informed decision. In this current concepts narrative review, we provide a comprehensive overview of the current knowledge on the anatomy, biomechanics, clinical and imaging diagnosis, nonsurgical and surgical treatment options, and outcomes after subtalar instability treatment.
Keywords: current concepts; instability; subtalar.
© The Author(s) 2021.
Conflict of interest statement
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Ashton-Miller JA, Ottaviani RA, Hutchinson C, Wojtys EM. What best protects the inverted weight-bearing ankle against further inversion? Evertor muscle strength compares favorably with shoe height, athletic tape, and 3 orthoses. Am J Sports Med. 1996;24(6):800–809. - PubMed
-
- Attarian DE, McCrackin HJ, DeVito DP, McElhaney JH, Garrett WE, Jr. Biomechanical characteristics of human ankle ligaments. Foot Ankle. 1985;6(2):54–58. - PubMed
-
- Aynardi M, Pedowitz DI, Raikin SM. Subtalar instability. Foot Ankle Clin. 2015;20(2):243–252. - PubMed
