

Dynamics and Predictors of Mortality Due to Candidemia Caused by Different Candida Species: Comparison of Intensive Care Unit-Associated Candidemia (ICUAC) and Non-ICUAC
- PMID: 34436136
- PMCID: PMC8397010
- DOI: 10.3390/jof7080597
Dynamics and Predictors of Mortality Due to Candidemia Caused by Different Candida Species: Comparison of Intensive Care Unit-Associated Candidemia (ICUAC) and Non-ICUAC
Abstract
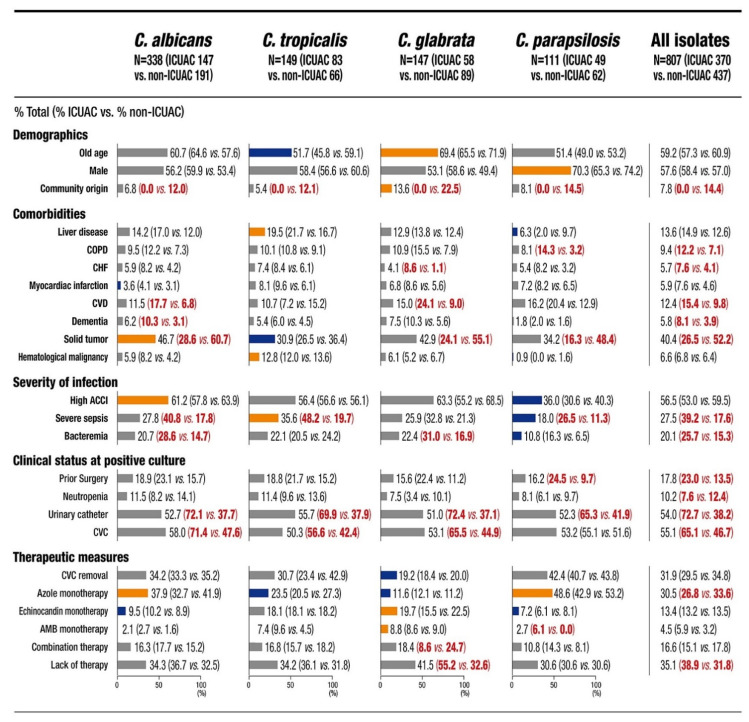
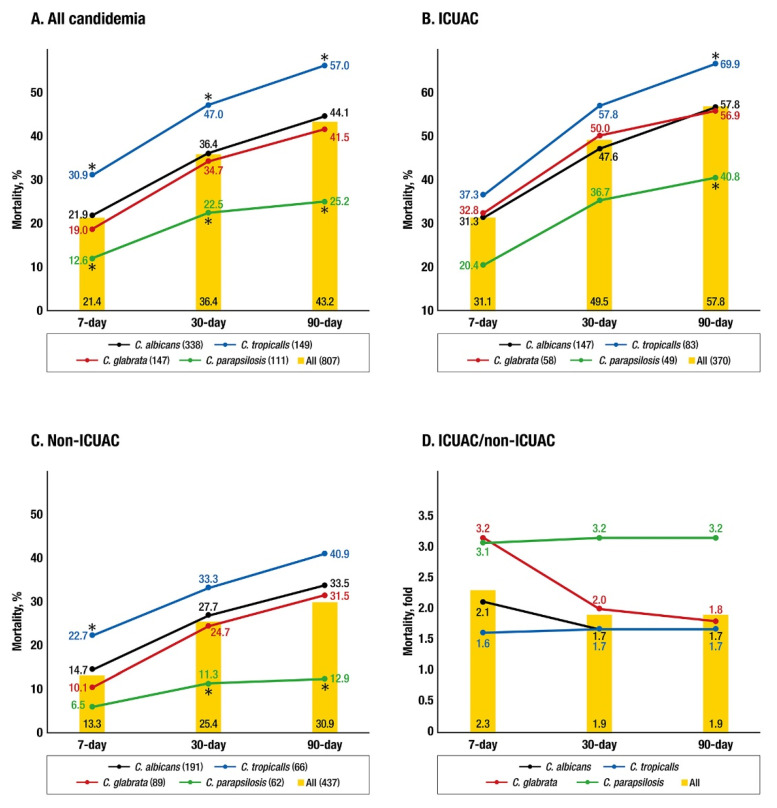
We investigated mortality and predictors of mortality due to intensive care unit-associated candidemia (ICUAC) versus non-ICUAC by Candida species. This study included all candidemia cases in 11 hospitals from 2017 to 2018 in South Korea. The all-cause mortality rates in all 370 patients with ICUAC were approximately twofold higher than those in all 437 patients with non-ICUAC at 7 days (2.3-fold, 31.1%/13.3%), 30 days (1.9-fold, 49.5%/25.4%), and 90 days (1.9-fold, 57.8%/30.9%). Significant species-specific associations with 7- and 30-day ICUAC-associated mortality were not observed. Multivariate analysis revealed that ICU admission was an independent predictor of Candida glabrata (OR, 2.07-2.48) and Candida parapsilosis-associated mortality (OR, 6.06-11.54). Fluconazole resistance was a predictor of C. glabrata-associated mortality (OR, 2.80-5.14). Lack (less than 3 days) of antifungal therapy was the strongest predictor of 7-day mortality due to ICUAC caused by Candida albicans (OR, 18.33), Candida tropicalis (OR, 10.52), and C. glabrata (OR, 21.30) compared with 30- and 90-day mortality (OR, 2.72-6.90). C. glabrata ICUAC had a stronger association with lack of antifungal therapy (55.2%) than ICUAC caused by other species (30.6-36.7%, all p < 0.05). Most predictors of mortality associated with ICUAC were distinct from those associated with non-ICUAC and were mediated by Candida species.
Keywords: Candida species; ICU; candidemia; lack of antifungal therapy; mortality.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Pappas P.G., Rex J.H., Lee J., Hamill R.J., Larsen R.A., Powderly W., Kauffman C.A., Hyslop N., Mangino J.E., Chapman S., et al. A prospective observational study of candidemia: Epidemiology, therapy, and influences on mortality in hospitalized adult and pediatric patients. Clin. Infect. Dis. 2003;37:634–643. doi: 10.1086/376906. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
