

Applicability of the Leiden Convention and the Lipton Classification in Patients with a Single Coronary Artery in the Setting of Congenital Heart Disease
- PMID: 34436235
- PMCID: PMC8397023
- DOI: 10.3390/jcdd8080093
Applicability of the Leiden Convention and the Lipton Classification in Patients with a Single Coronary Artery in the Setting of Congenital Heart Disease
Abstract
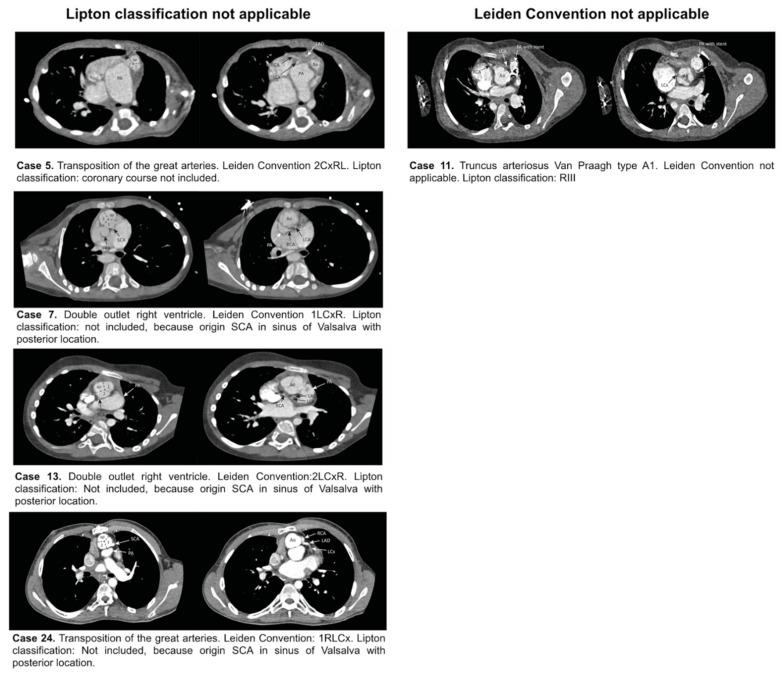
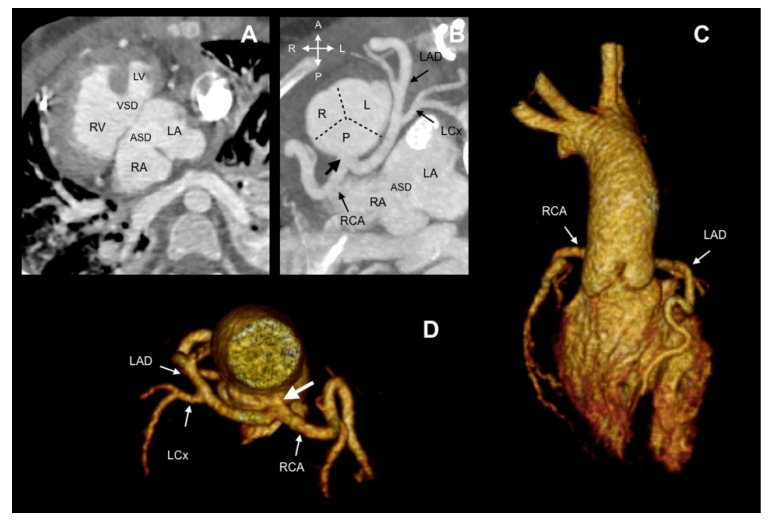
In single coronary artery (SCA) anatomy, all coronary tributaries arise from a single ostium, providing perfusion to the entire myocardium. Coronary classification systems can facilitate the description of SCA anatomy. Aim: Evaluation of the applicability of Lipton classification and the Leiden Convention coronary coding system in SCA. Methods: All patients (n = 6209) who underwent computed tomography (CT) scanning between 2014 and 2018 were retrospectively examined for the presence of SCA and classified, according to Lipton classification and the Leiden Convention coronary coding system. Results: The prevalence of SCA was 0.51% (32/6209). Twenty-eight patients (87.5%) had coexisting congenital heart disease (CHD), most frequently pulmonary atresia (9/32, 28.1%). Ten patients (10/32, 31.25%) could not be classified with either the Leiden Convention or Lipton classification (pulmonary atresia n = 9, common arterial trunk (CAT) n = 1). In one case with CAT, Lipton classification, but not the Leiden Convention, could be applied. In two cases with the transposition of the great arteries and in two cases of double outlet right ventricle, the Leiden Convention, but not the Lipton classification, could be applied. Conclusions: Both classifications are useful to detail information about SCA. As Lipton classification was not developed for structural heart disease cases, in complex CHD with abnormal position of the great arteries, the Leiden Convention is better applicable. The use of both systems is limited in pulmonary atresia. In this scenario, it is better to provide a precise description of the coronary origin and associated characteristics that might affect treatment and prognosis.
Keywords: Leiden Convention coronary coding system; Lipton classification; congenital heart disease; coronary artery anatomy; single coronary artery.
Conflict of interest statement
All authors declare no conflict of interest. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Figures




References
-
- Gittenberger-de Groot A.C., Sauer U., Oppenheimer-Dekker A., Quaegebeur J. Coronary arterial anatomy in transposition of the great arteries: A morphologic study. Pediatr. Cardiol. 1983;4:15–24.
-
- Gittenberger-de Groot A.C., Koenraadt W.M.C., Bartelings M.M., Bökenkamp R., DeRuiter M.C., Hazekamp M.G., Bogers A., Quaegebeur J.M., Schalij M.J., Vliegen H.W., et al. Coding of coronary arterial origin and branching in congenital heart disease: The modified Leiden Convention. J. Thorac. Cardiovasc. Surg. 2018;156:2260–2269. doi: 10.1016/j.jtcvs.2018.08.009. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
