

Comparison of Midterm Outcomes Associated With Aspirin and Ticagrelor vs Aspirin Monotherapy After Coronary Artery Bypass Grafting for Acute Coronary Syndrome
- PMID: 34436610
- PMCID: PMC8391102
- DOI: 10.1001/jamanetworkopen.2021.22597
Comparison of Midterm Outcomes Associated With Aspirin and Ticagrelor vs Aspirin Monotherapy After Coronary Artery Bypass Grafting for Acute Coronary Syndrome
Abstract
Importance: Guidelines recommend dual antiplatelet therapy after coronary artery bypass grafting (CABG) for patients with acute coronary syndrome (ACS). However, the evidence for these recommendations is weak.
Objective: To compare midterm outcomes after CABG in patients with ACS treated postoperatively with acetylsalicylic acid (ASA) and ticagrelor or with ASA monotherapy.
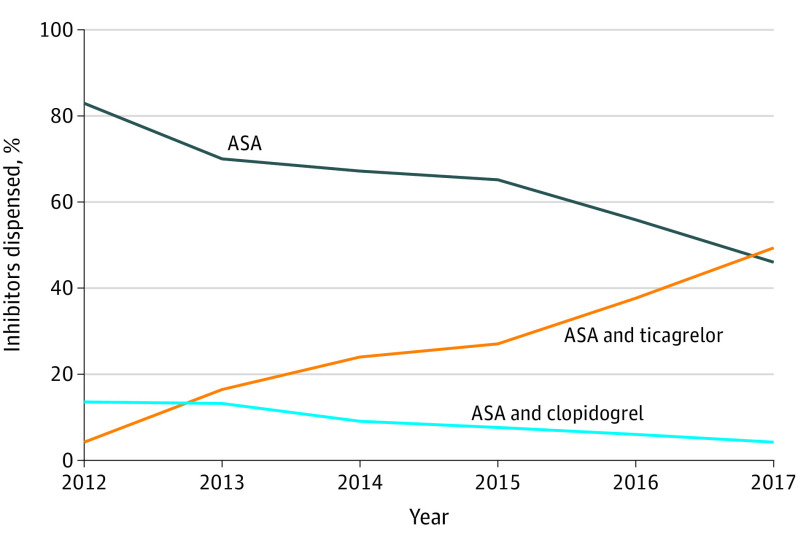
Design, setting, and participants: This cohort study used merged data from several national registries of Swedish patients who were diagnosed with ACS and subsequently underwent CABG. All included patients underwent isolated CABG in Sweden between 2012 and 2017 with an ACS diagnosis less than 6 weeks before the procedure, survived 14 days after discharge from hospital, and were treated postoperatively with ASA plus ticagrelor or ASA monotherapy. A multivariable Cox regression model was used for the main analysis, and propensity score-matched models were performed as sensitivity analysis. Data were analyzed between May and September 2020.
Exposures: Postoperative antiplatelet treatment, defined as filled prescriptions, with either ASA and ticagrelor or ASA only.
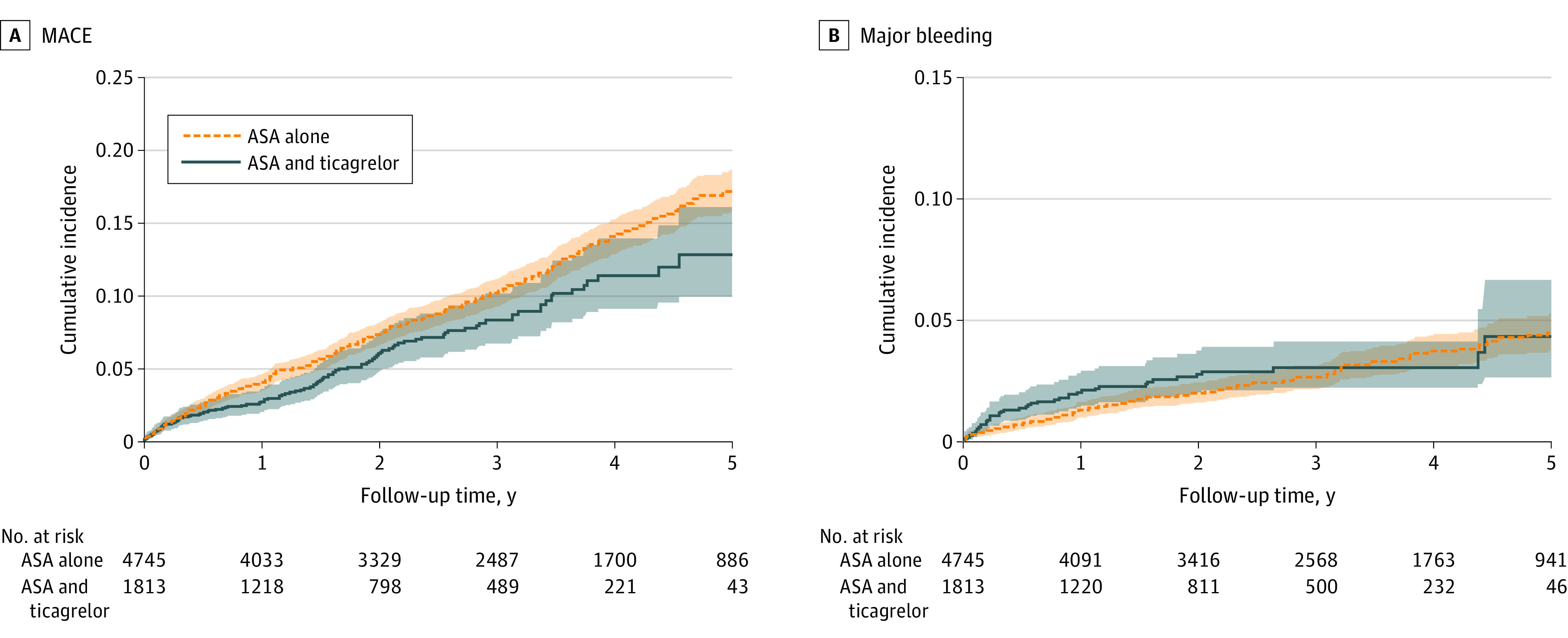
Main outcomes and measures: Major adverse cardiovascular events (MACE), defined as all-cause mortality, myocardial infarction, and stroke, and major bleeding, at 12 months and at the end of follow-up.
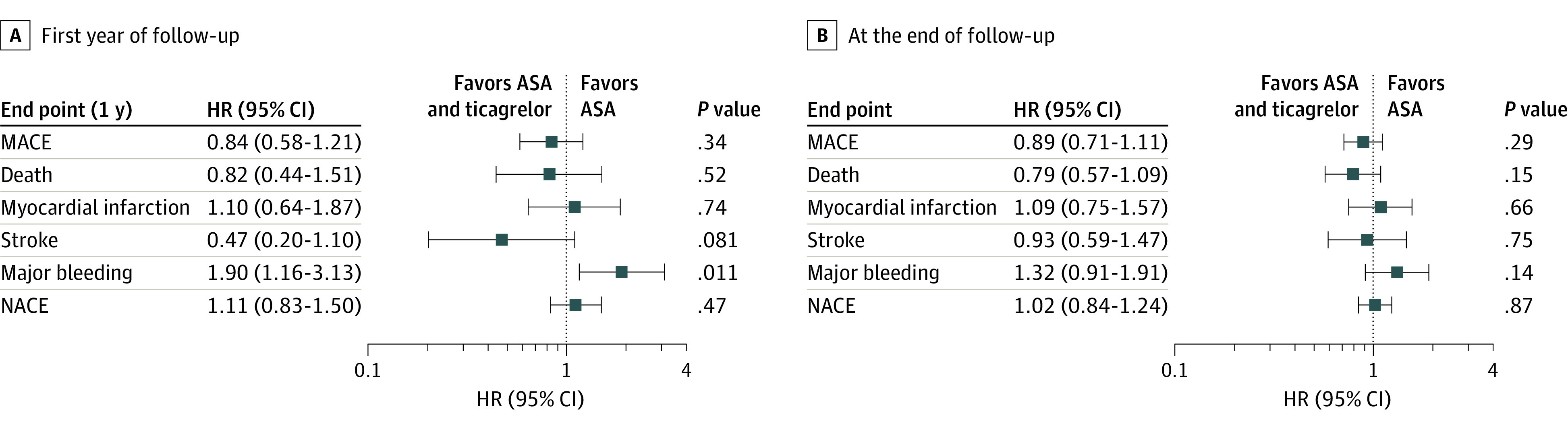
Results: A total of 6558 patients (5281 [80.5%] men; mean [SD] age at surgery, 67.6 [9.3] years) were included; 1813 (27.6%) were treated with ASA plus ticagrelor and 4745 (72.4%) were treated with ASA monotherapy. Crude MACE rate was 3.0 per 100 person years (95% CI, 2.5-3.6 per 100 person years) in the ASA plus ticagrelor group and 3.8 per 100 person years (95% CI, 3.5-4.1 per 100 person years) in the ASA group. After adjustment, there was no significant difference in MACE risk between ASA plus ticagrelor vs ASA only, neither during the first 12 months (adjusted hazard ratio [aHR], 0.84; 95% CI, 0.58-1.21; P = .34) or during total follow-up (aHR, 0.89; 95% CI, 0.71-1.11; P = .29). The use of ASA plus ticagrelor was associated with a significantly increased risk for major bleeding during the first 12 months (aHR, 1.90; 95% CI, 1.16-3.13; P = .011). Sensitivity analyses confirmed the results.
Conclusions and relevance: In patients with ACS who survived 2 weeks after CABG, no significant difference in the risk of death or ischemic events could be demonstrated between ASA plus ticagrelor and patients treated with ASA only, while the risk for major bleeding was higher in patients treated with ASA plus ticagrelor. Sufficiently powered prospective randomized trials comparing different antiplatelet therapy strategies after CABG are warranted.
Conflict of interest statement
Figures
Similar articles
-
Bleeding risk in patients prescribed dual antiplatelet therapy and triple therapy after coronary interventions: the ADAPTT retrospective population-based cohort studies.Health Technol Assess. 2023 May;27(8):1-257. doi: 10.3310/MNJY9014. Health Technol Assess. 2023. PMID: 37435838 Free PMC article.
-
Safety of Preoperative Use of Ticagrelor With or Without Aspirin Compared With Aspirin Alone in Patients With Acute Coronary Syndromes Undergoing Coronary Artery Bypass Grafting.JAMA Cardiol. 2016 Nov 1;1(8):921-928. doi: 10.1001/jamacardio.2016.3028. JAMA Cardiol. 2016. PMID: 27653165 Clinical Trial.
-
Antiplatelet therapy after coronary artery bypass surgery: five year follow-up of randomised DACAB trial.BMJ. 2024 Jun 11;385:e075707. doi: 10.1136/bmj-2023-075707. BMJ. 2024. PMID: 38862179 Free PMC article. Clinical Trial.
-
Should dual antiplatelet therapy be used in patients following coronary artery bypass surgery? A meta-analysis of randomized controlled trials.BMC Surg. 2015 Oct 14;15:112. doi: 10.1186/s12893-015-0096-z. BMC Surg. 2015. PMID: 26467661 Free PMC article. Review.
-
Association of Dual Antiplatelet Therapy With Ticagrelor With Vein Graft Failure After Coronary Artery Bypass Graft Surgery: A Systematic Review and Meta-analysis.JAMA. 2022 Aug 9;328(6):554-562. doi: 10.1001/jama.2022.11966. JAMA. 2022. PMID: 35943473 Free PMC article.
Cited by
-
Revealing the Process of Vein Graft Failure: A Panoramic Review from Etiology Analysis to Mechanism Explanation and Treatment Strategy.Cardiovasc Drugs Ther. 2025 May 29. doi: 10.1007/s10557-025-07711-3. Online ahead of print. Cardiovasc Drugs Ther. 2025. PMID: 40439962 Review.
-
Antithrombotic Therapy in Elderly Patients with Acute Coronary Syndromes.J Clin Med. 2022 May 26;11(11):3008. doi: 10.3390/jcm11113008. J Clin Med. 2022. PMID: 35683397 Free PMC article. Review.
-
The Management and Antithrombotic Strategies of Patients with Coronary Artery Disease and High Bleeding Risk.Curr Cardiol Rep. 2023 Jul;25(7):669-680. doi: 10.1007/s11886-023-01893-8. Epub 2023 Jun 7. Curr Cardiol Rep. 2023. PMID: 37285104 Review.
-
Postdischarge major bleeding, myocardial infarction, and mortality risk after coronary artery bypass grafting.Heart. 2024 Mar 22;110(8):569-577. doi: 10.1136/heartjnl-2023-323394. Heart. 2024. PMID: 38148160 Free PMC article.
-
Antiplatelet therapy around CABG: the latest evidence.Curr Opin Cardiol. 2023 Nov 1;38(6):484-489. doi: 10.1097/HCO.0000000000001078. Epub 2023 Sep 21. Curr Opin Cardiol. 2023. PMID: 37751394 Free PMC article. Review.
References
-
- Valgimigli M, Bueno H, Byrne RA, et al. ; ESC Scientific Document Group; ESC Committee for Practice Guidelines (CPG); ESC National Cardiac Societies . 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: the task force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2018;39(3):213-260. doi:10.1093/eurheartj/ehx419 - DOI - PubMed
-
- Held C, Asenblad N, Bassand JP, et al. . Ticagrelor versus clopidogrel in patients with acute coronary syndromes undergoing coronary artery bypass surgery: results from the PLATO (Platelet Inhibition and Patient Outcomes) trial. J Am Coll Cardiol. 2011;57(6):672-684. doi:10.1016/j.jacc.2010.10.029 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
