

Wearables-based walking program in addition to usual physiotherapy care for the management of patients with low back pain at medium or high risk of chronicity: A pilot randomized controlled trial
- PMID: 34437607
- PMCID: PMC8389429
- DOI: 10.1371/journal.pone.0256459
Wearables-based walking program in addition to usual physiotherapy care for the management of patients with low back pain at medium or high risk of chronicity: A pilot randomized controlled trial
Abstract
Background: Although chronic low back pain (LBP) is a leading cause of disability and accounts for large costs, none of the available conventional treatments are clearly more favourable in treating people at increased risk of chronicity.
Objectives: To examine the feasibility and initial efficacy of a wearables-based walking intervention in addition to usual physiotherapy care in people with LBP at risk of chronicity.
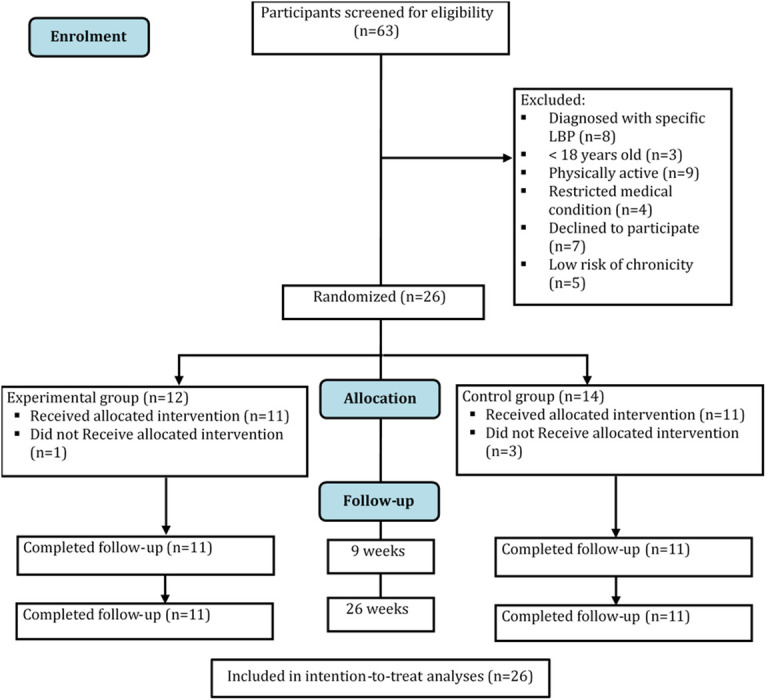
Methods: Twenty-six adult participants, diagnosed with non-specific LBP with medium or high risk of chronicity, were recruited from physiotherapy private practices. Participants were randomized into usual physiotherapy care (control, n = 14) and usual physiotherapy care plus a wearables-based walking intervention (experimental, n = 12). The intervention duration was 8 weeks. Feasibility outcomes included recruitment rate, adherence to the intervention, dropout rate, and serious adverse events reporting rate. Other outcomes included disability and pain (primary); and physical activity level, daily walking steps, depression, pain catastrophizing and fear of movement (secondary). The outcomes were assessed at baseline, post-intervention and 26 weeks post-randomization follow-up.
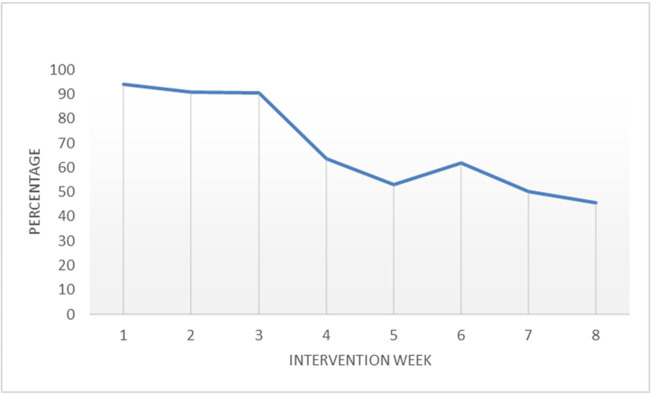
Results: Adherence of experimental participants with the prescribed walking program was moderate. Four participants dropped out during the intervention, and no serious adverse events were reported. Participants in the experimental group showed significant improvement in pain at 26 weeks (β = -0.38; 95% confidence interval (CI) -0.66, -0.10; P = .013), compared with the control group. No between-group differences were found for disability at any time point and pain immediately post-intervention. Experimental participants demonstrated post-intervention improvement in light-intensity (β = 156.71; 95% CI 86.79, 226.64; P < .001), moderate-intensity physical activity (β = 0.46; 95% CI 0.12, 0.80; P = .012), and daily walking steps (β = 7099.13; 95% CI 4522.93, 9675.32; P < .001). Experimental participants demonstrated post-intervention increase in pain catastrophizing (β = 0.52, 95% CI 0.18, 0.86; P = .006). No between-group differences were found for pain catastrophizing at 26 weeks and other secondary outcomes.
Conclusion: Usual physiotherapy care plus a wearables-based walking intervention program was safe and moderately feasible, and provided significant reduction in pain at 26 weeks as well as increasing the total volume of light- and moderate-intensity physical activity, and daily walking steps immediately post-intervention.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Vos T, Abajobir AA, Abate KH, Abbafati C, Abbas KM, Abd-Allah F, et al.. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211–59. doi: 10.1016/S0140-6736(17)32154-2 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
