

Plate Fixation for Irreducible Proximal Humeral Fractures in Children and Adolescents-A Single-Center Case Series of Six Patients
- PMID: 34438526
- PMCID: PMC8393487
- DOI: 10.3390/children8080635
Plate Fixation for Irreducible Proximal Humeral Fractures in Children and Adolescents-A Single-Center Case Series of Six Patients
Abstract
Background: Recommended treatment for severely displaced proximal humeral fractures in children is the closed reduction and percutaneous fixation by K-wires or intramedullary nailing.
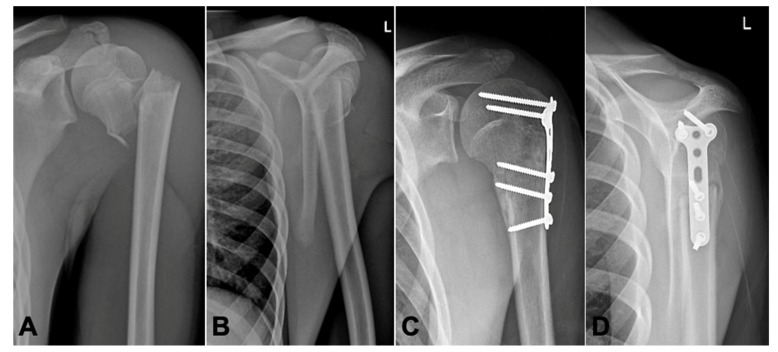
Methods: From January 2016 to January 2017 6, 21 children/adolescents (range 8 to 16 years) with proximal humeral fractures were treated surgically for severe displacement. In these six patients, several attempts of closed reduction were unsuccessful, and an open reduction was performed. The humeral head was fixed with a 3.5 mm T-plate without affecting the growth plate. Plate removal was performed at a mean interval of 132 days after initial surgery. Two years after initial surgery, the clinical outcome was assessed by the Constant-Murley score and QuickDASH score (including sport/music and work) and the shoulder joint was evaluated with a standardized sonographic examination for the rotator cuff and the conjoint tendon.
Results: In all six patients, dorsal displacement of the fracture was irreducible due to the interposition of tendinous or osseous structures. Intraoperatively, the interposed structures were the long biceps tendon in two, periosteal tissue in two, a bony fragment in one, and the long biceps tendon together with the conjoint tendon in one case. At mean follow-up of 26 months (range 22 months to 29 months), patients showed very good clinical results with an excellent mean Constant-Murley score of 97.5 (range 91 to 100) and mean QuickDASH score (including sport/music and work) of 5.5 (range 0-20.8). An X-ray follow-up 6 weeks after surgery demonstrated early consolidation and correct alignment in all patients. A sonographic evaluation at 2 years post injury showed that the biceps and the conjoined tendon were intact in all patients.
Conclusions: If a proximal humeral fracture is not reducible by closed means, a tissue entrapment (most likely biceps tendon) should be considered. Treatment with an open reduction and plate fixation yields very good clinical and radiological results and preserves interposed structures as the biceps and conjoint tendon.
Keywords: ORIF; biceps; children; humerus fracture; plate fixation; proximal humeral fracture; tissue entrapment.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Neer Fractures of the proximal humeral epiphyseal plate. Clin. Orthop. Relat. Res. 1965;41:24–31. - PubMed
LinkOut - more resources
Full Text Sources
