

Vitreoretinal Lymphoma
- PMID: 34439078
- PMCID: PMC8394064
- DOI: 10.3390/cancers13163921
Vitreoretinal Lymphoma
Abstract
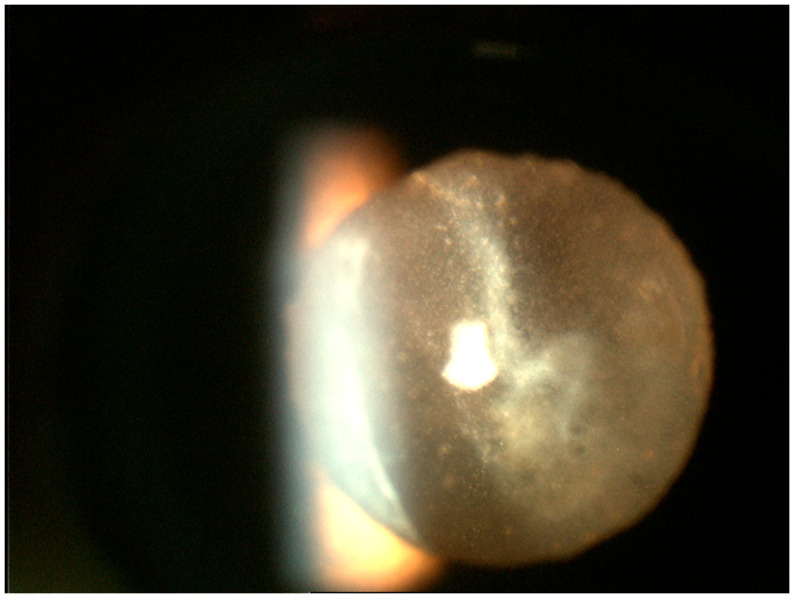
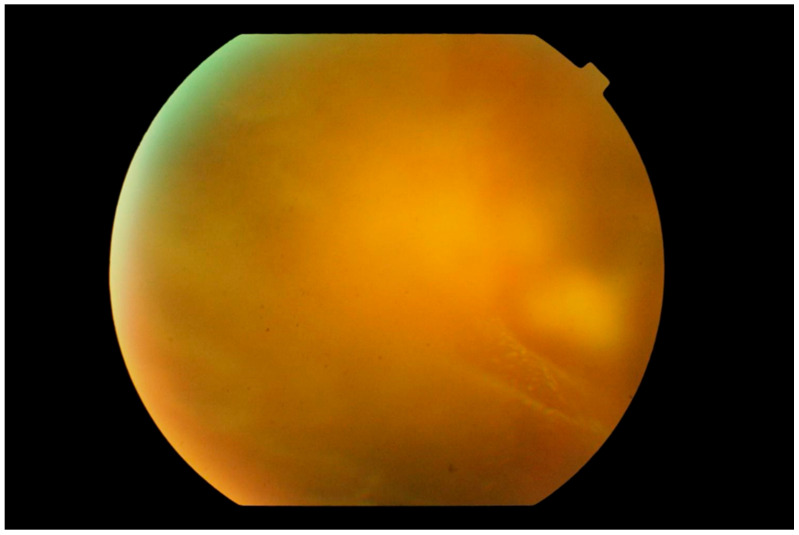
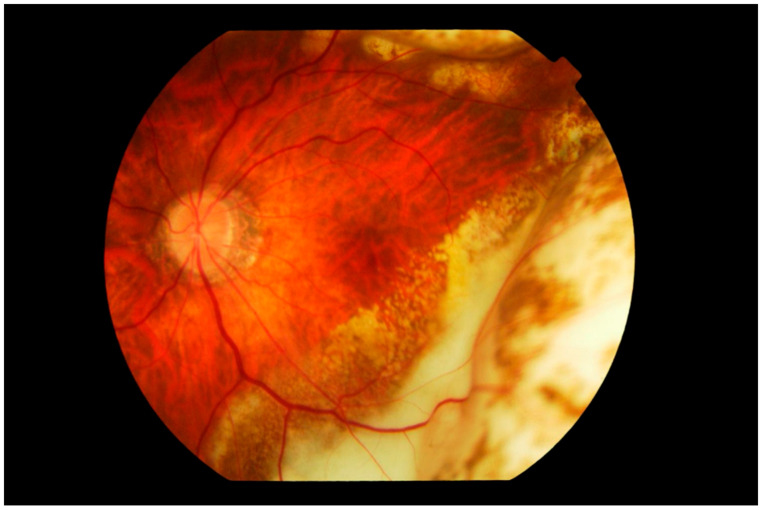
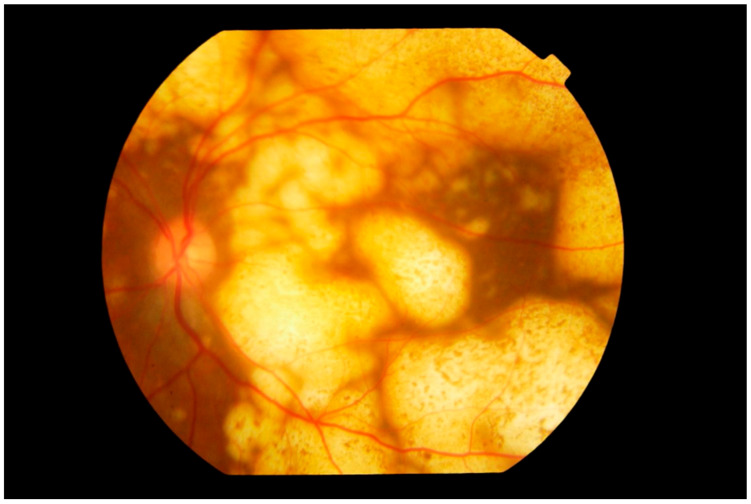
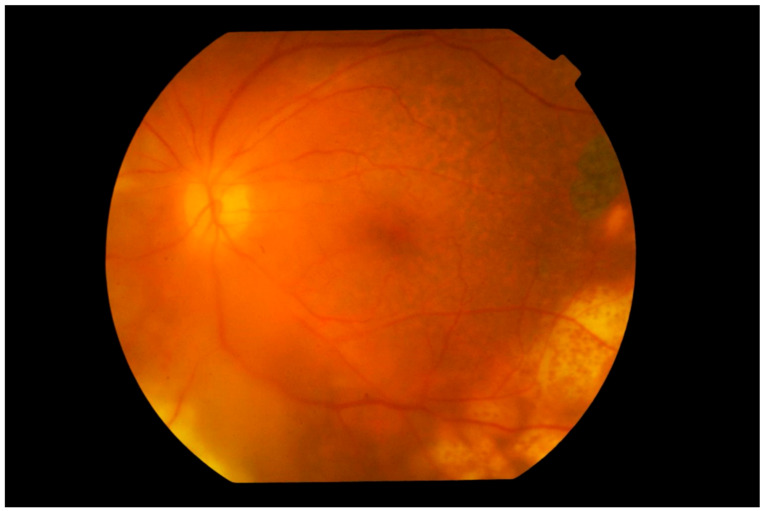
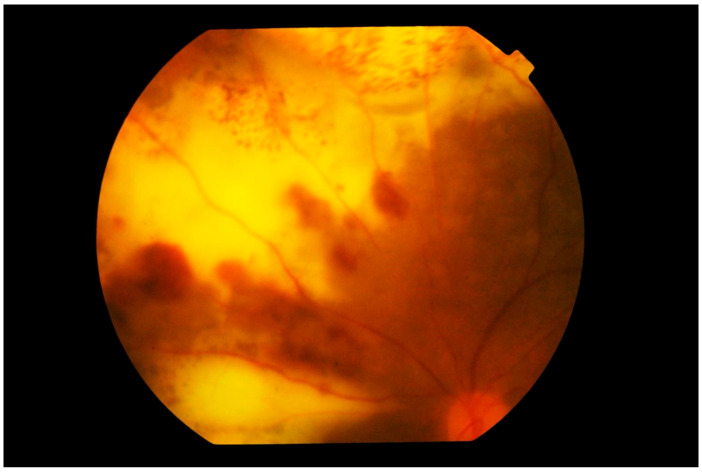
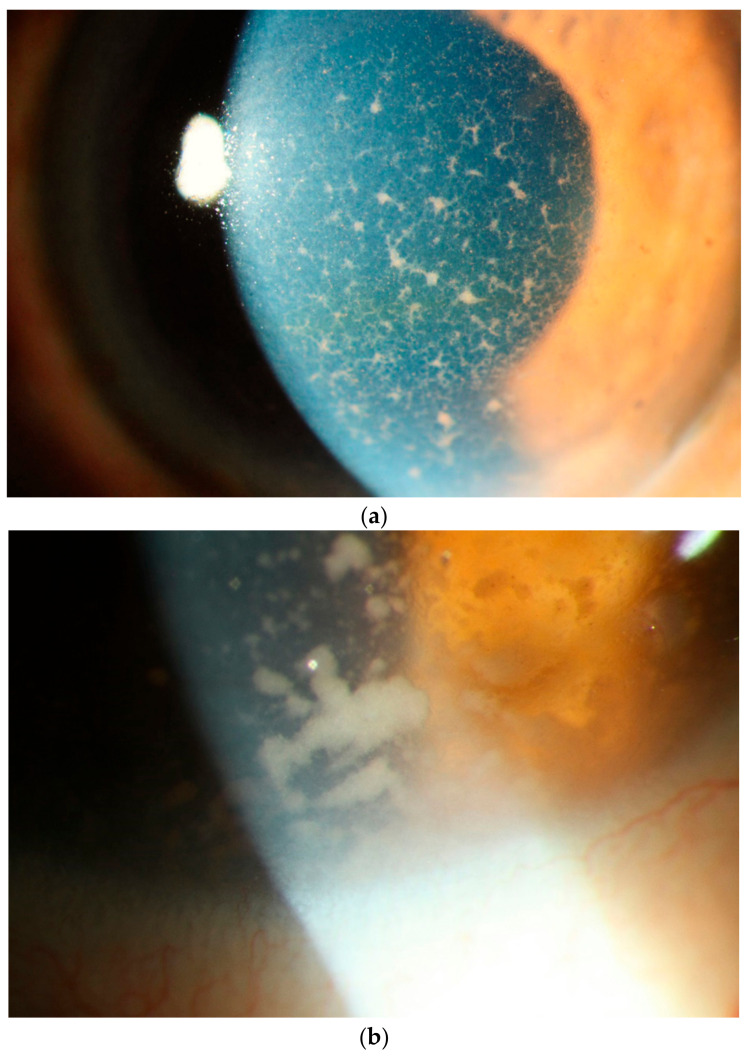
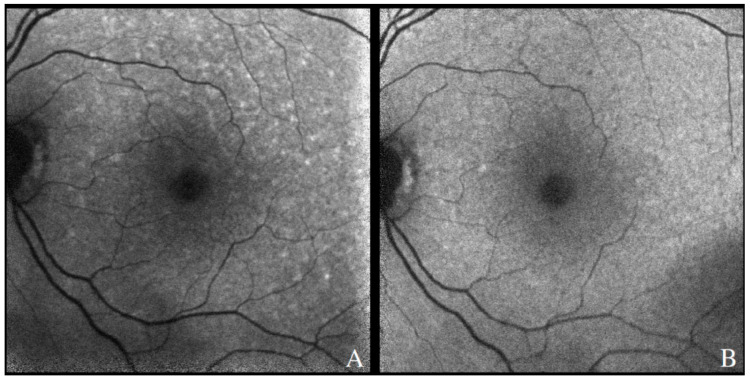
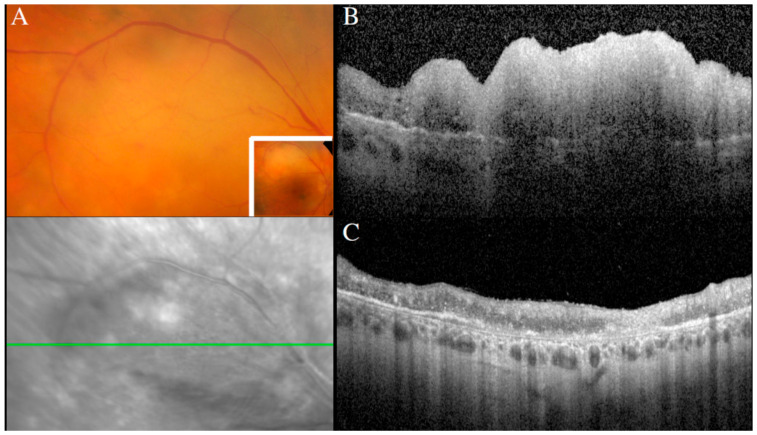
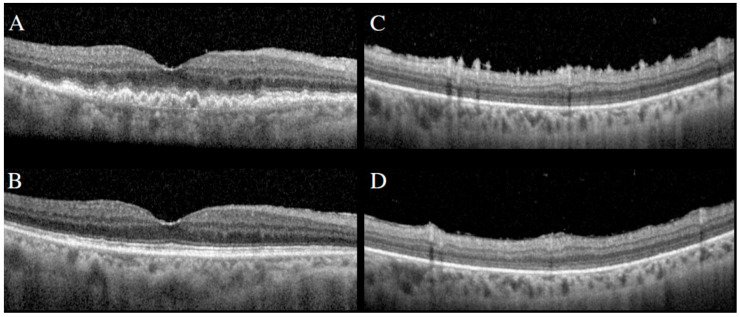
Vitreoretinal lymphoma (VRL) is a rare variant of primary central nervous system lymphoma (PCNSL), mostly of diffuse large B cell lymphoma, which affects the retina and/or the vitreous with or without optic nerve involvement. The disease course is aggressive. Up to 90% of the patients develop central nervous system lymphoma within one year. The diagnosis of VRL is challenging due to nonspecific chronic and relapsing uveitis and is made by anterior chamber tab or vitreous aspirate biopsy. There is no established treatment protocol for VRL patients with bilateral involvement without CNS involvement. There are suggestions to use only intravitreal chemotherapy with methotrexate and/or rituximab. Alternatively, systemic high-dose MTX treatment or external beam radiotherapy is used. Further studies are needed to prove and confirm the prophylactic systemic therapy in preventing CNS involvement in limited VRL.
Keywords: CNS lymphoma; IL-10/IL-6 ratio; MYD88; methotrexate; vitreoretinal lymphoma.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
